

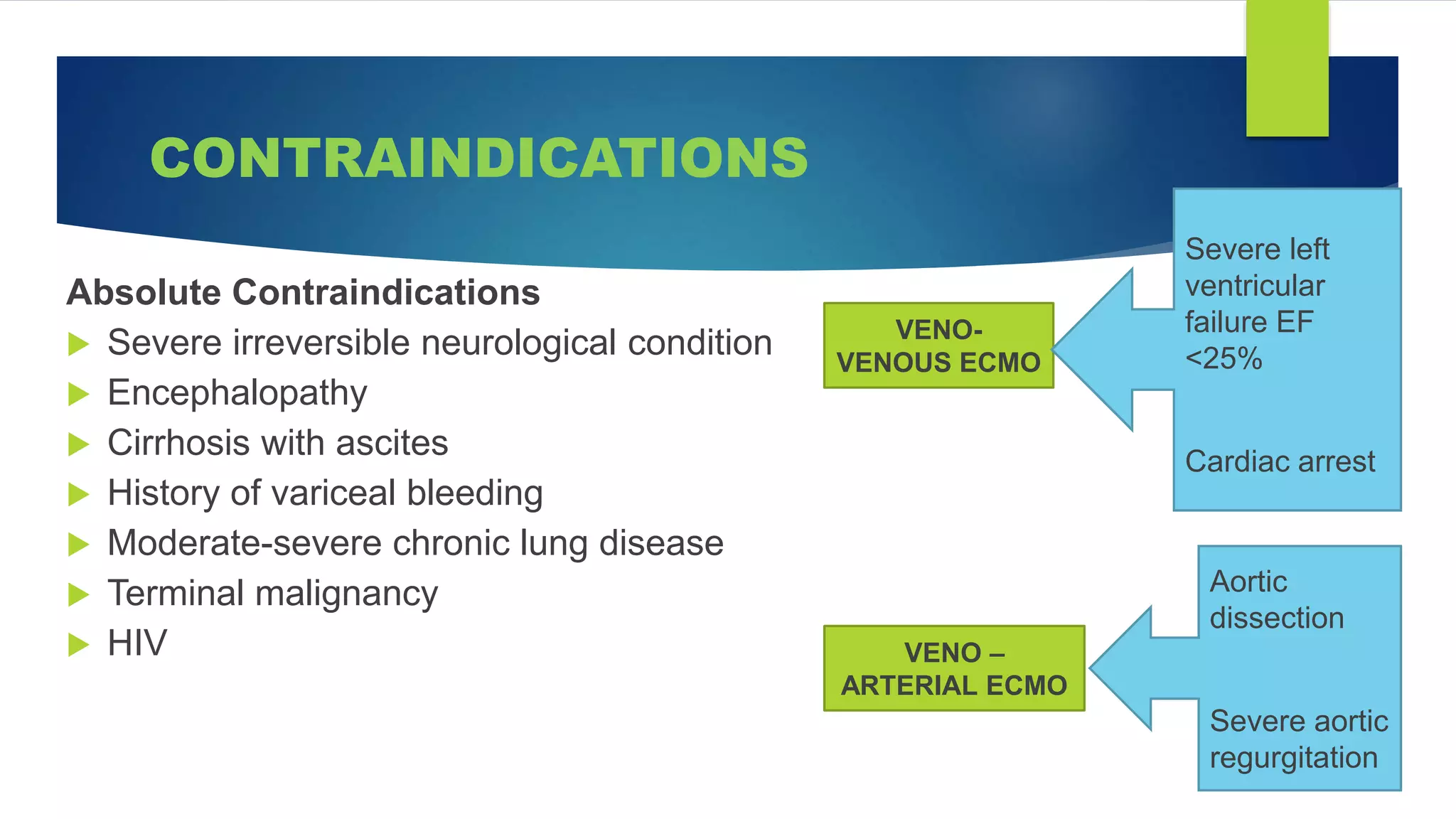




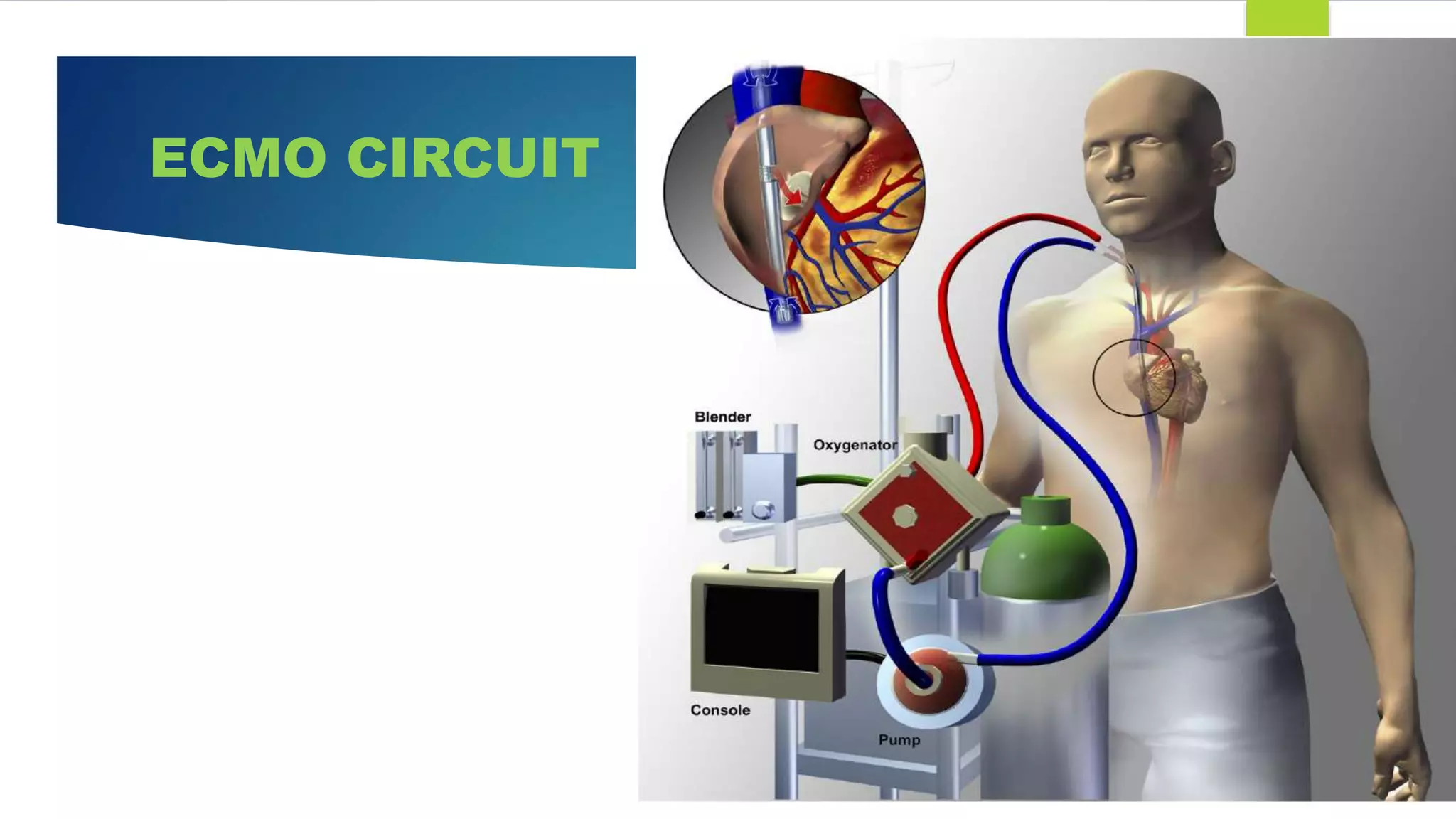










Extracorporeal membrane oxygenation (ECMO) is a life support technique that provides cardiac and respiratory assistance by circulating blood through an oxygenator, primarily used for patients with severe cardiac or pulmonary failure unresponsive to conventional treatments. The document outlines the history, indications, contraindications, types of ECMO, management protocols, complications, and recent research findings indicating that ECMO may improve survival rates and neurological outcomes compared to conventional CPR. Early detection is crucial for effective ECMO application to enhance patient survival outcomes.