Downloaded 204 times



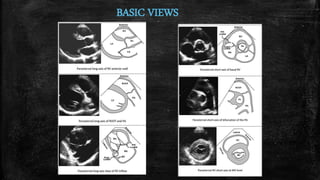
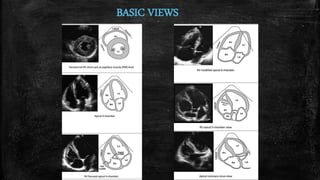

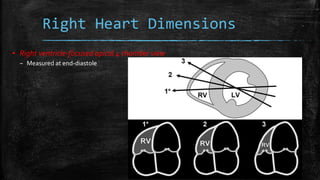
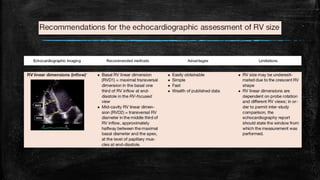
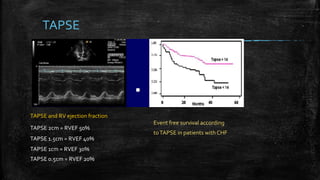
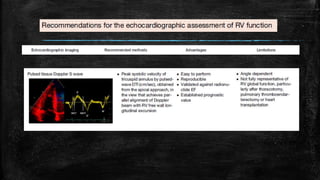
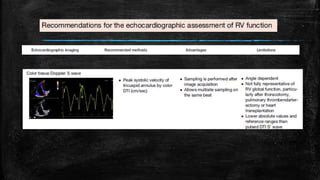
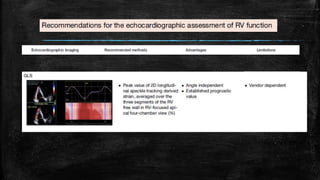
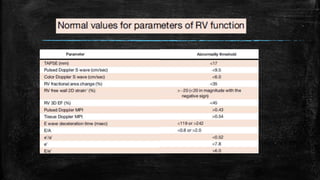
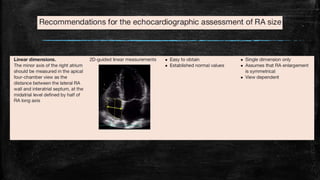
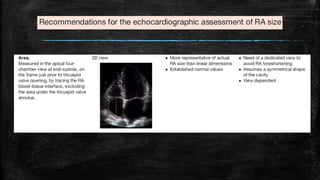
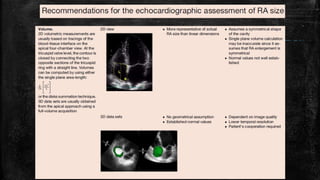

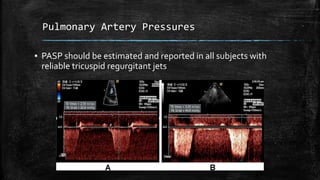

This document provides guidelines for assessing right heart structure and function using echocardiography. It describes the basic views needed to evaluate the right ventricle and atria. Key measurements are outlined such as ventricular dimensions, tricuspid annular plane systolic excursion (TAPSE), and inferior vena cava (IVC) size and collapse. Methods for estimating pulmonary artery pressures from tricuspid regurgitation are presented. The document recommends routinely reporting right ventricular size and function on echocardiograms.




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













