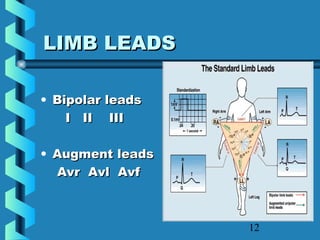
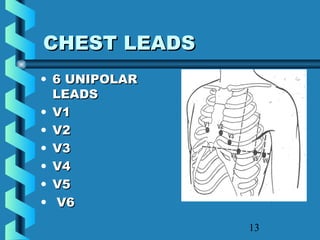
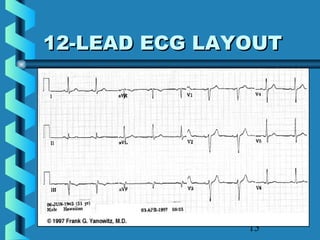
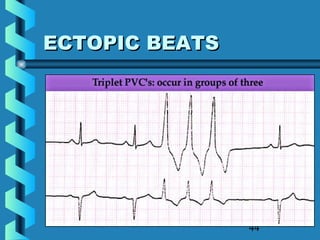
This document provides instructions for performing and interpreting a 12-lead electrocardiogram (ECG). It describes the proper procedure for electrode placement on the limbs and chest to produce the 12 leads. It also covers evaluating the ECG for correct lead placement, artifacts, and basic abnormalities like arrhythmias, ectopic beats, and critical values such as ST elevation. The overall goal is to produce high quality ECGs and correctly interpret basic findings.

































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
