Downloaded 545 times





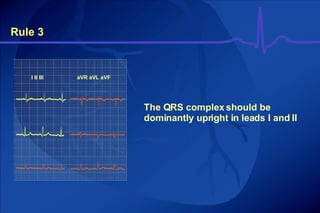


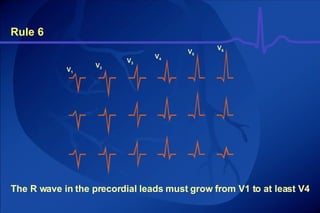

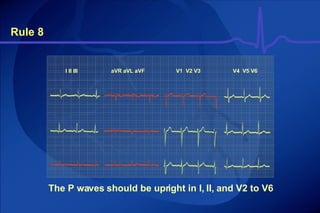
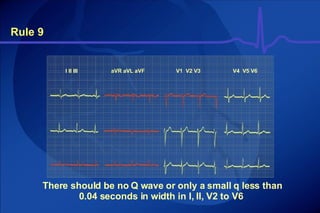


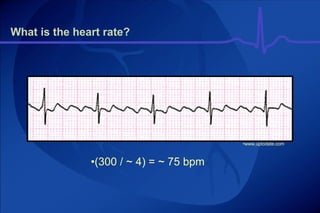




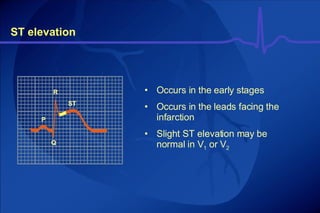

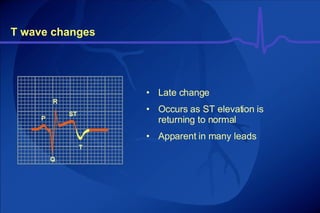
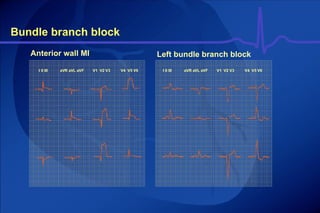

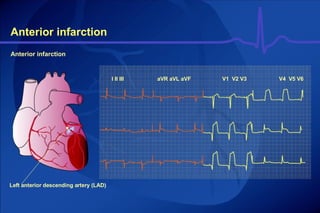
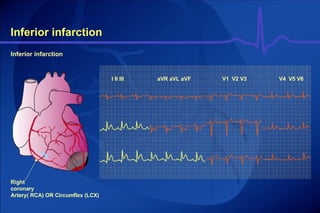





The document discusses electrocardiography (ECG) and how it is used to diagnose myocardial infarction (MI). It provides details on: 1) How 12 leads are used to view the heart electrically from different angles and locations, and which 10 electrodes are used. 2) The typical signs seen on an ECG during an MI, including ST segment elevation, pathological Q waves, reduced R waves, and inverted T waves. 3) The sequence of ECG changes that occur during an evolving MI, from initial onset through later stages. 4) How different leads on the ECG can indicate the location of an infarct, such as anterior vs inferior walls.