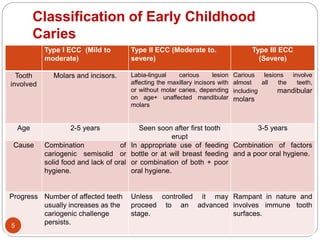
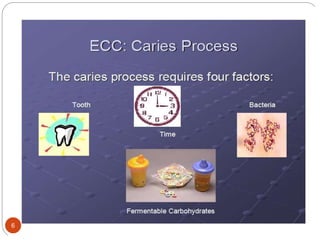
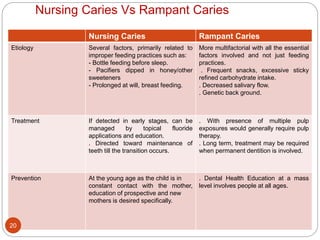
The document discusses early childhood caries, defining it as dental caries affecting children under 6 years old. It describes the causes as prolonged exposure to fermentable carbohydrates from bottle feeding or breastfeeding coupled with poor oral hygiene. The management involves restoring existing cavities, counseling parents on improving feeding practices and oral hygiene, and applying topical fluorides to arrest the caries process.
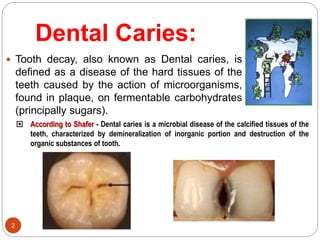
![EARLY CHILDHOOD CARIES
it is a unique pattern of dental caries in very young children due to
prolonged and improper feeding habits.
Terminologies
-Nursing Caries
-Nursing Bottle Caries/ Mouth/ Syndrome
-Night Bottle Syndrome
-Baby Bottle Tooth Decay
-Milk Bottle Syndrome
-Tooth Cleaning Neglect
-Infant & Early Childhood Decay
-RIECDO [Rampant Infant and Early Childhood Dental
Decay]
-Maternally Derived Streptococcus Mutants Disease
[MDSMD]
-Early Childhood Caries [ECC]
3](https://image.slidesharecdn.com/earlychildhoodcaries-220427094640/85/Early-childhood-caries-ppt-3-320.jpg)














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











