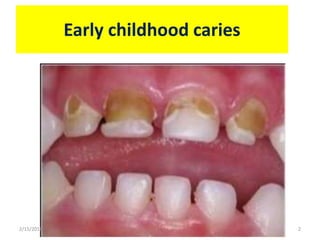
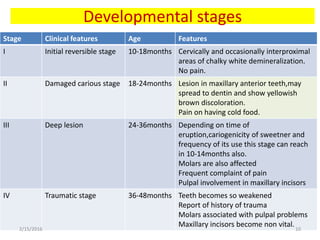
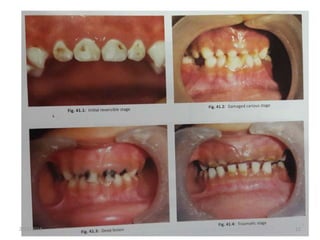
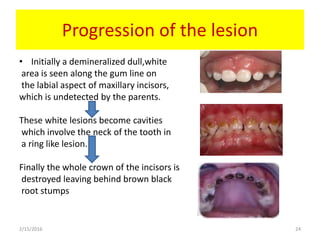
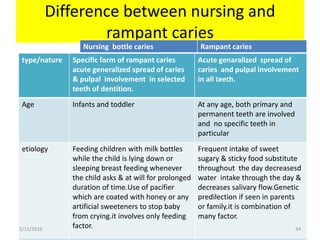
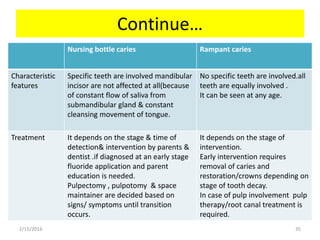
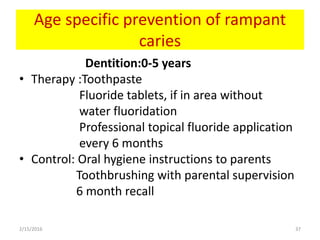
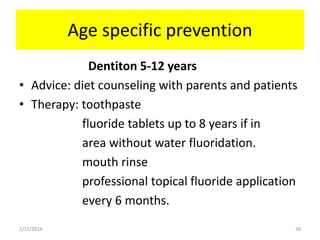
Early childhood caries (ECC), also known as nursing bottle caries, is a multifactorial disease caused by the presence of cariogenic bacteria like Streptococcus mutans transmitted from mother to child combined with frequent consumption of fermentable carbohydrates, especially from prolonged bottle feeding. ECC affects primary teeth, typically beginning with maxillary anterior teeth. If left untreated, lesions can progress rapidly, leading to pulp involvement, pain, and tooth loss. Prevention focuses on reducing sugar intake, proper oral hygiene, and eliminating bottle use in bed.