Download as PDF, PPTX


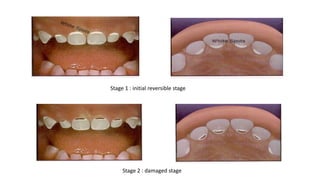
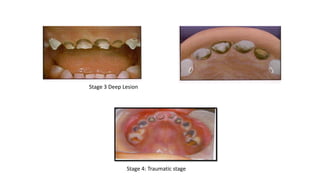
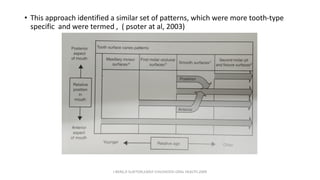
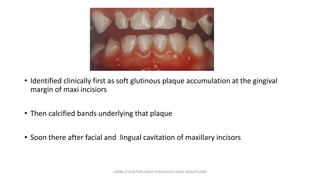
















This document discusses early childhood caries (ECC), providing a history of terminology used to describe it and definitions that have been proposed. ECC was first described in 1862 and various terms like "nursing bottle caries" and "baby bottle tooth decay" were used. In 1999, it was defined as presence of decay, missing, or filled tooth surfaces in a child under age 6. Risk factors and classifications of ECC are discussed. Prevention strategies are also mentioned, including establishing dental homes, anticipatory guidance, and dietary recommendations.