Downloaded 262 times






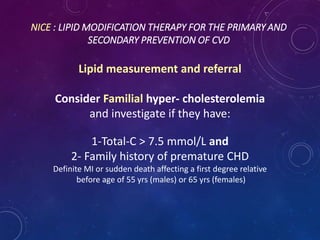
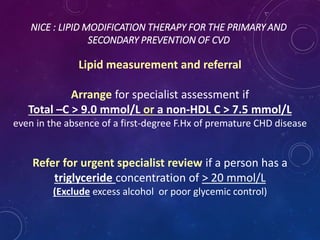

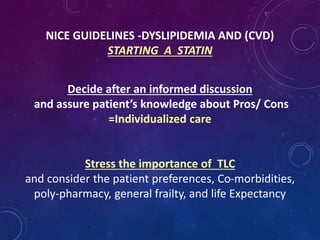
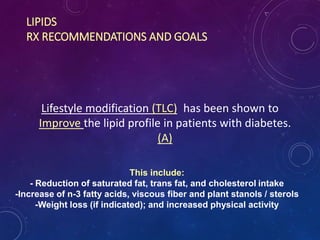


![NICE
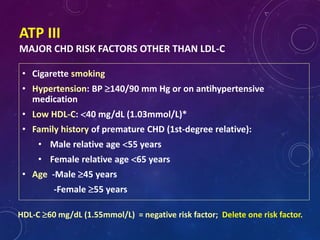
COMBINATION RX
Do not routinely offer Fibrates and
Do not offer Nicotinic acid (niacin) or Bile acid sequestrants (anion
exchange resins) or omega-3 fatty acid compounds for the
prevention of CVD to any of the following group of patients :
-Treated for primary prevention
-Treated for secondary prevention
-With CKD
-With type 1 DM
-With type 2 DM
[new 2014]](https://image.slidesharecdn.com/dyslipdemiaslideshare-150225105648-conversion-gate01/85/Dyslipdemia-Guidelines-Head-to-Head-56-320.jpg)



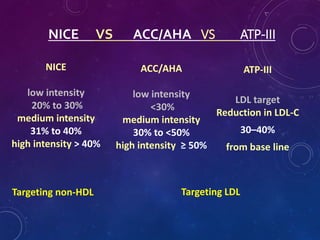

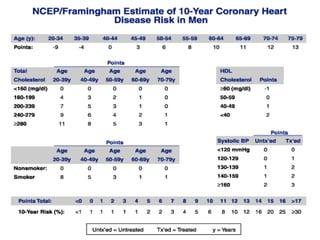
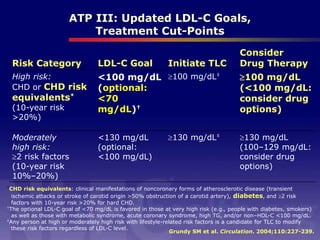
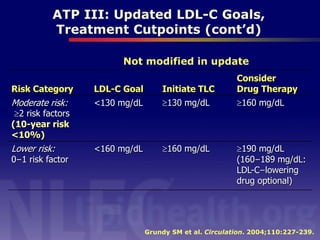
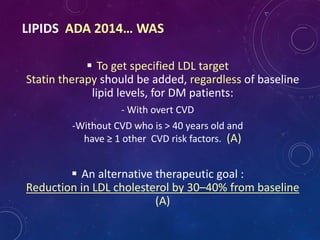
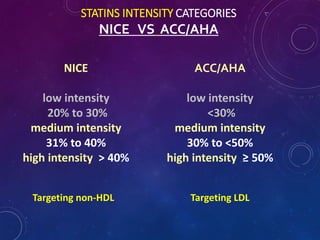
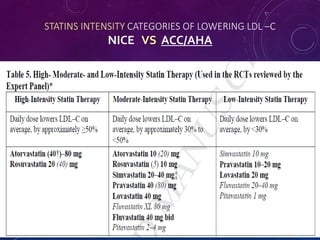
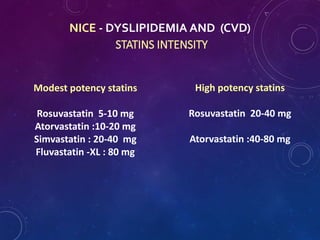
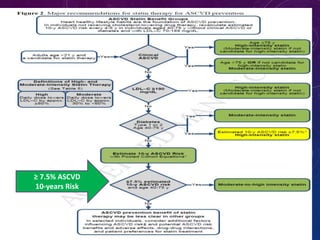
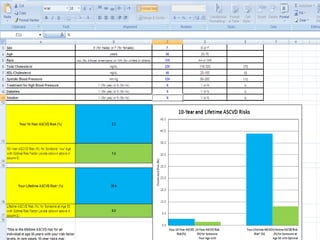
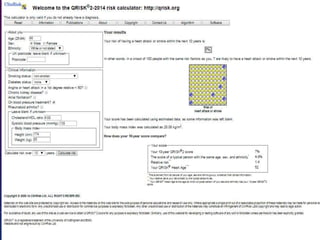
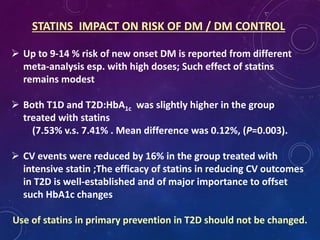
This document provides guidelines for the assessment and management of dyslipidemia from several major organizations. It discusses risk assessment tools for cardiovascular disease from ATP III, ADA, ACC/AHA, and QRISK2. It also compares statin intensity categories between NICE and ACC/AHA guidelines. The document recommends lifestyle modification as first-line treatment and the use of high-intensity statins for primary and secondary prevention of CVD according to the guidelines of NICE, ADA, and ACC/AHA.






































![Dyslipidemia [Compatibility Mode]](https://cdn.slidesharecdn.com/ss_thumbnails/dyslipidemiacompatibilitymode-090922105322-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)































































