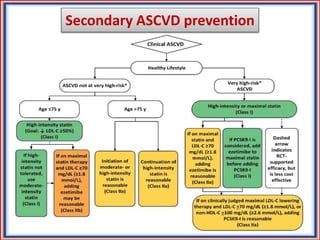
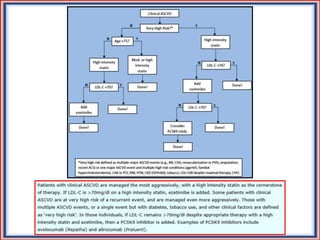
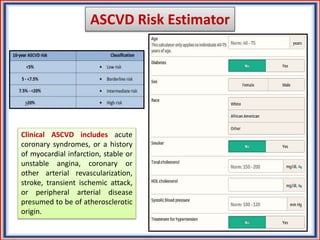
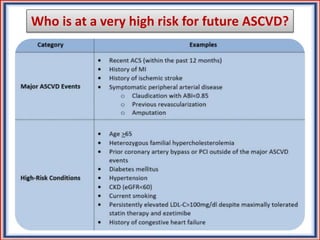
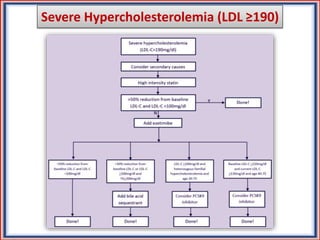
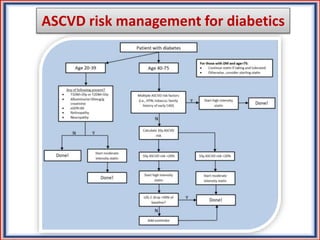

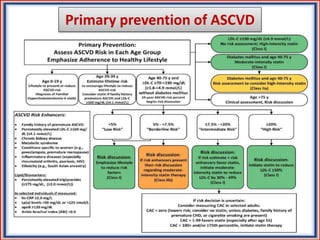
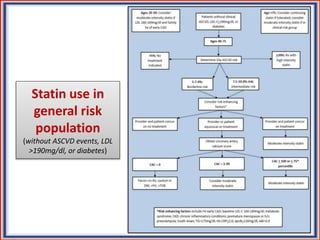
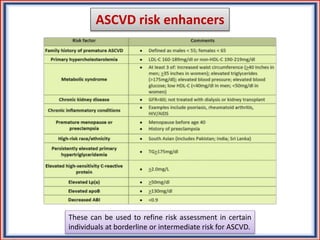


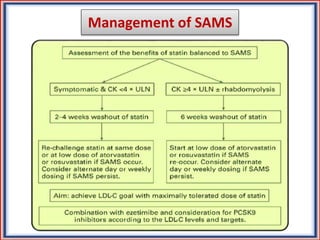
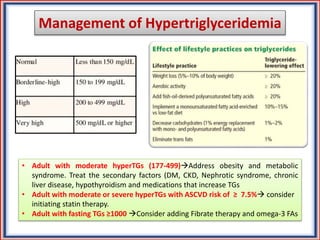
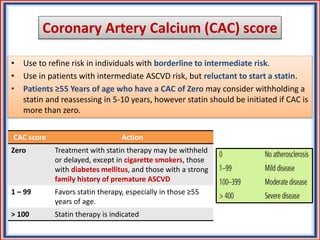
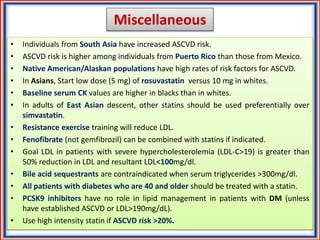
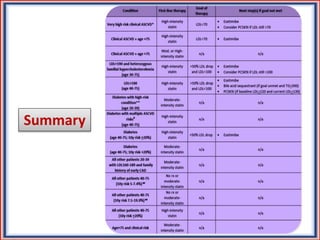


The document provides guidelines for cholesterol management and cardiovascular disease (CVD) risk assessment. It discusses guidelines for measuring cholesterol and lipid levels, calculating LDL and VLDL values, and assessing CVD risk. It recommends starting moderate- or high-intensity statin therapy for most adults aged 40-75 years with diabetes or LDL ≥70 mg/dL. For those without diabetes but with a CVD risk of 7.5% or higher, it recommends discussing statin therapy. The guidelines also provide recommendations for managing statin side effects, evaluating risk factors, and refining risk assessment using coronary artery calcium scoring. The main messages are to emphasize lifestyle changes, use high-intensity statins for high-risk patients, and consider patient risk























































































