![NICE
COMBINATION RX
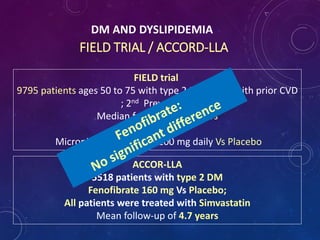
Do not routinely offer Fibrates
(Field trial & ACCORD –Lipid)
and
Do not offer Nicotinic acid (niacin) or Bile acid sequestrants (anion
exchange resins) or omega-3 fatty acid compounds for the
prevention of CVD to any of the following group of patients :
-Treated for primary prevention
-Treated for secondary prevention
-With CKD
-With type 1 DM
-With type 2 DM
[new 2014]](https://image.slidesharecdn.com/dmdyslipdemiaslideshare-151128172542-lva1-app6891/85/Diabetic-Dyslipidemia-Slide-Share-52-320.jpg)



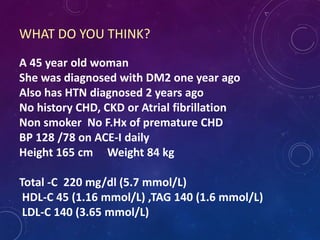
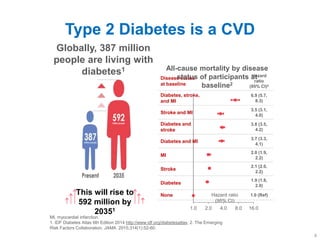
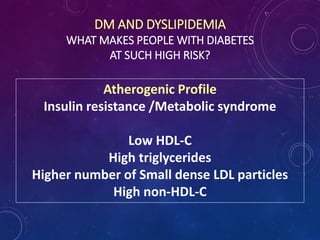
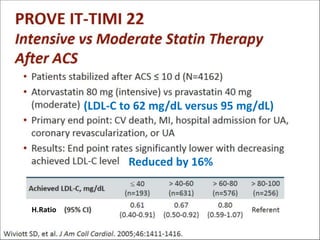
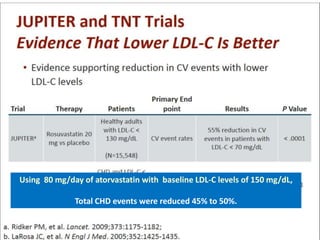
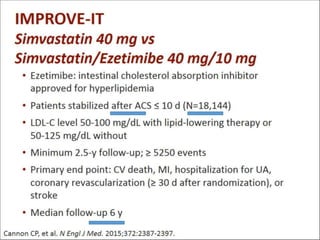
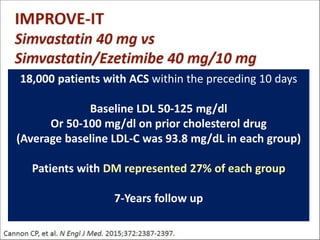
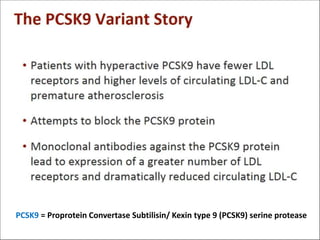
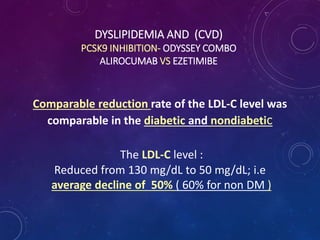
The document discusses diabetic dyslipidemia and its treatment strategies, focusing on a case of a 45-year-old woman with Type 2 diabetes and dyslipidemia. It highlights the importance of statin therapy for both primary and secondary prevention of cardiovascular disease in diabetic patients, emphasizing LDL-c targets and intensity of treatment based on various guidelines. The document also outlines the various risk factors for cardiovascular disease and the efficacy of different medications including statins, ezetimibe, and monoclonal antibodies like PCSK9 inhibitors.































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






