Downloaded 93 times

![Leading Causes of Death: USA
• Number of deaths for leading causes of death
1. Heart disease: 647,457
2. Cancer: 599,108
3. Accidents (unintentional injuries): 169,936
4. Chronic lower respiratory diseases: 160,201
5. Stroke (cerebrovascular diseases):
146,383
6. Alzheimer’s disease: 121,404
7. Diabetes: 83,564
8. Influenza and pneumonia: 55,672
9. Nephritis, nephrotic syndrome, and nephrosis:
50,633
10. Intentional self-harm (suicide): 47,173
Deaths: Leading Causes for 2017, table 1 pdf icon[PDF- 2 MB]: CDC](https://image.slidesharecdn.com/dyslipidemiaapproach-201213235238/75/Dyslipidemia-approach-5-2048.jpg)


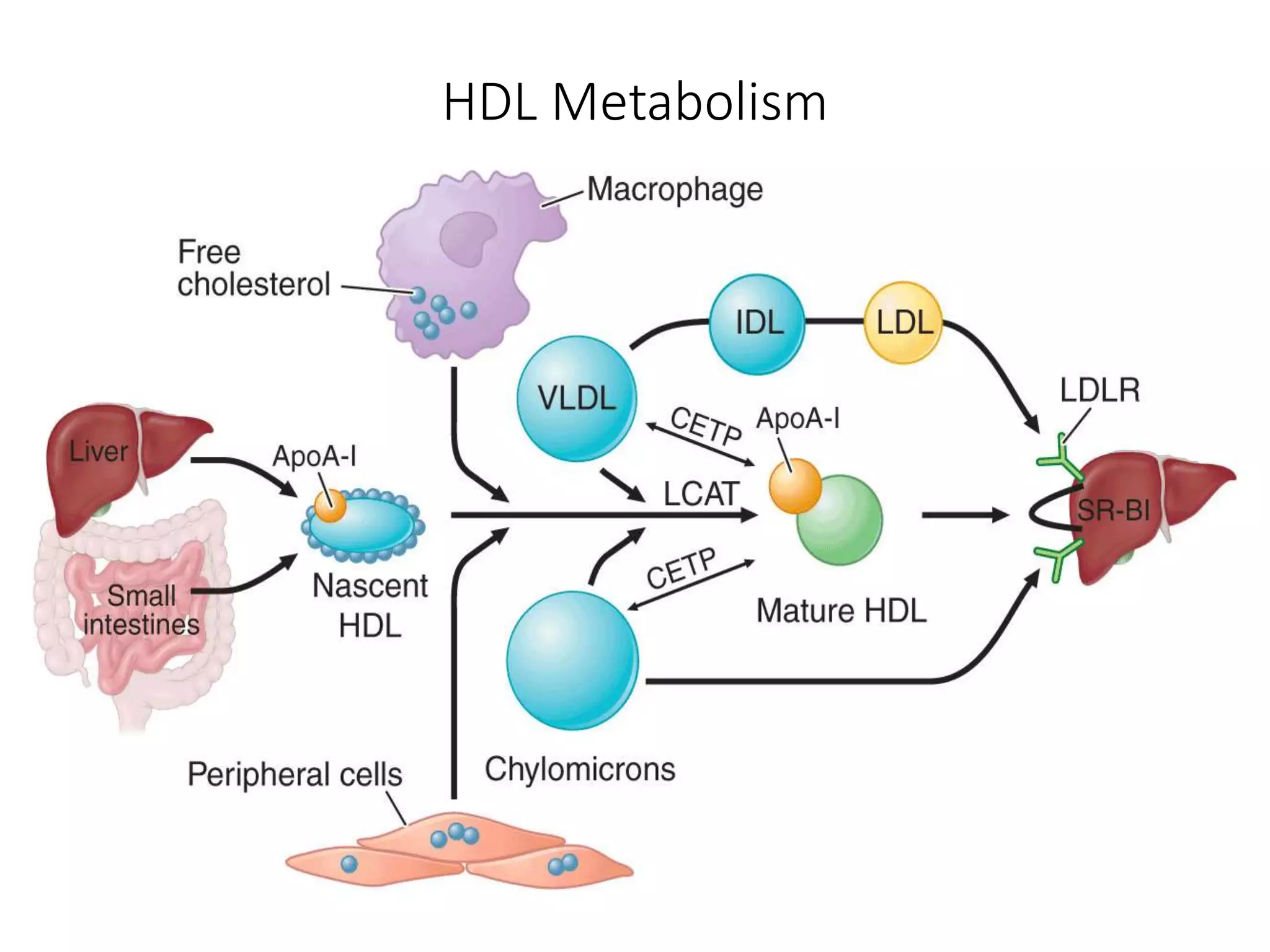


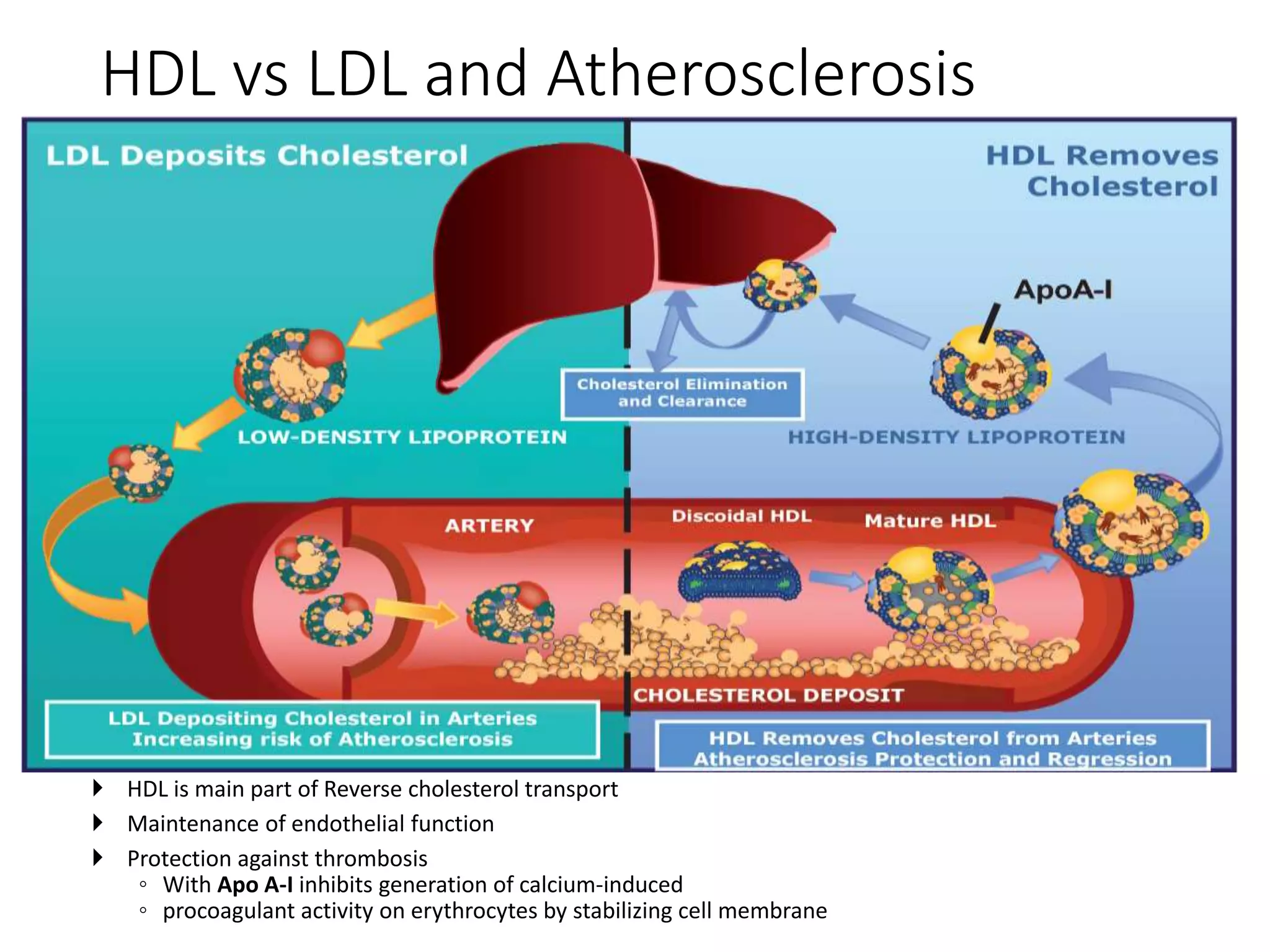
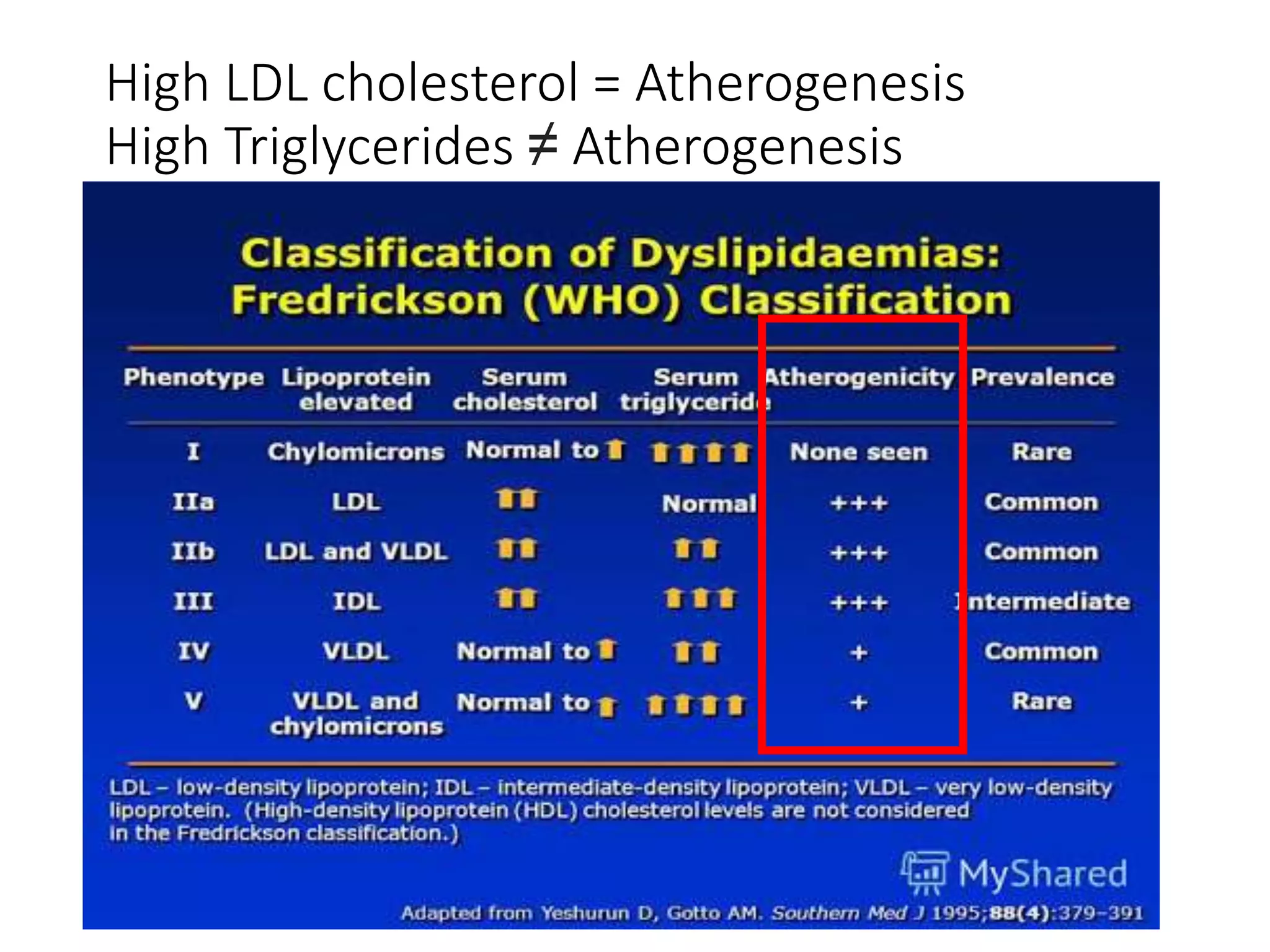

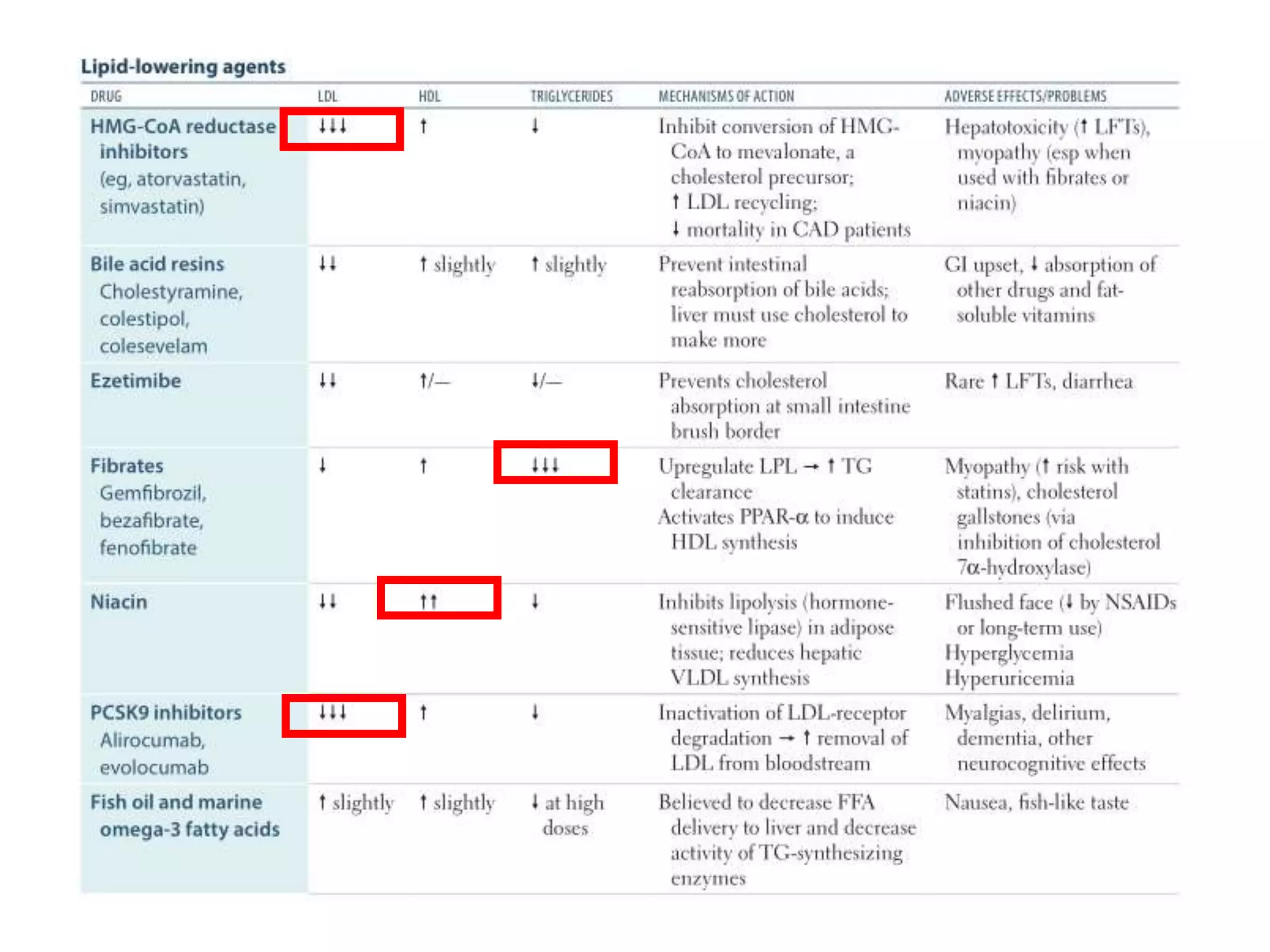










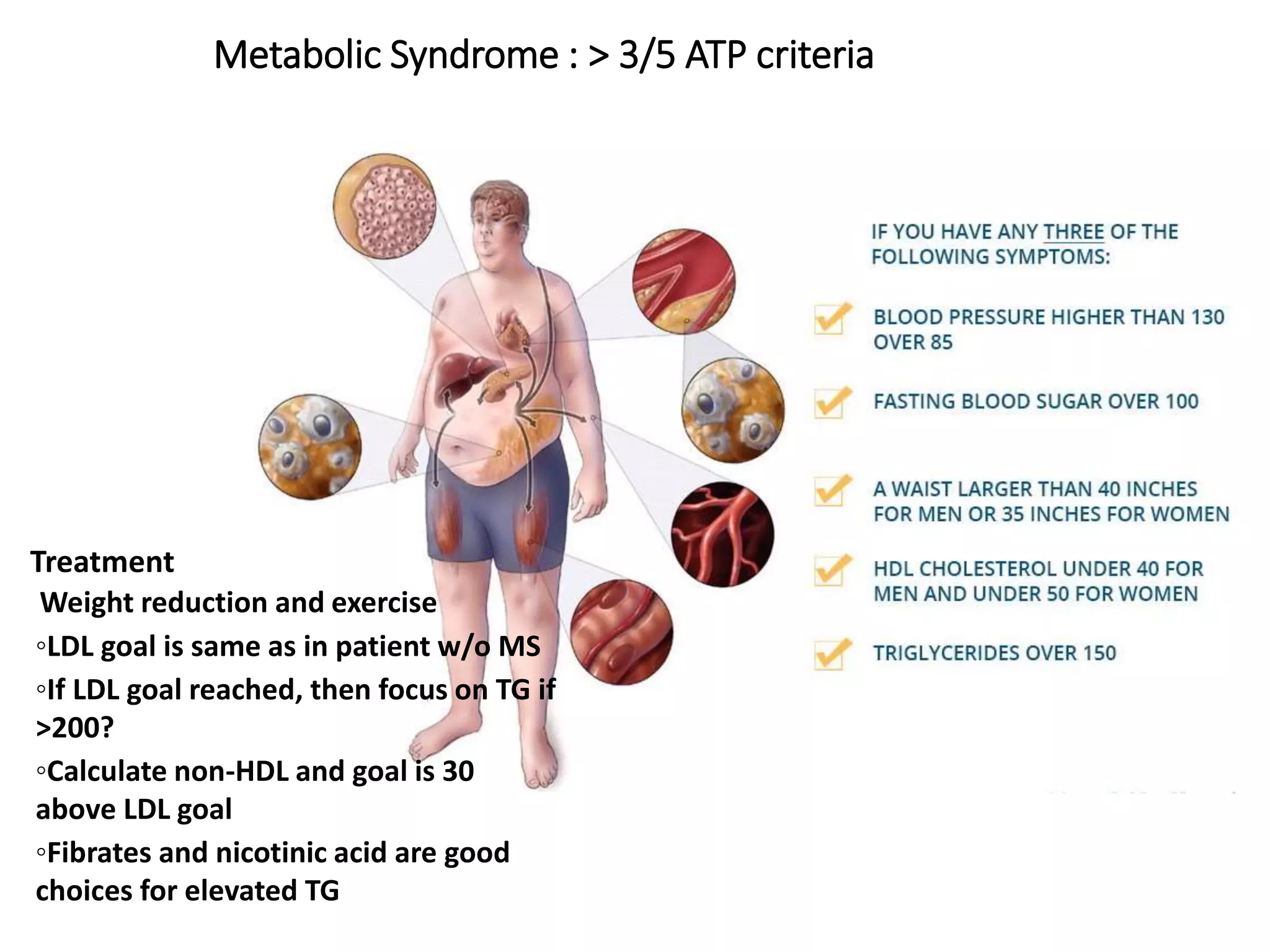






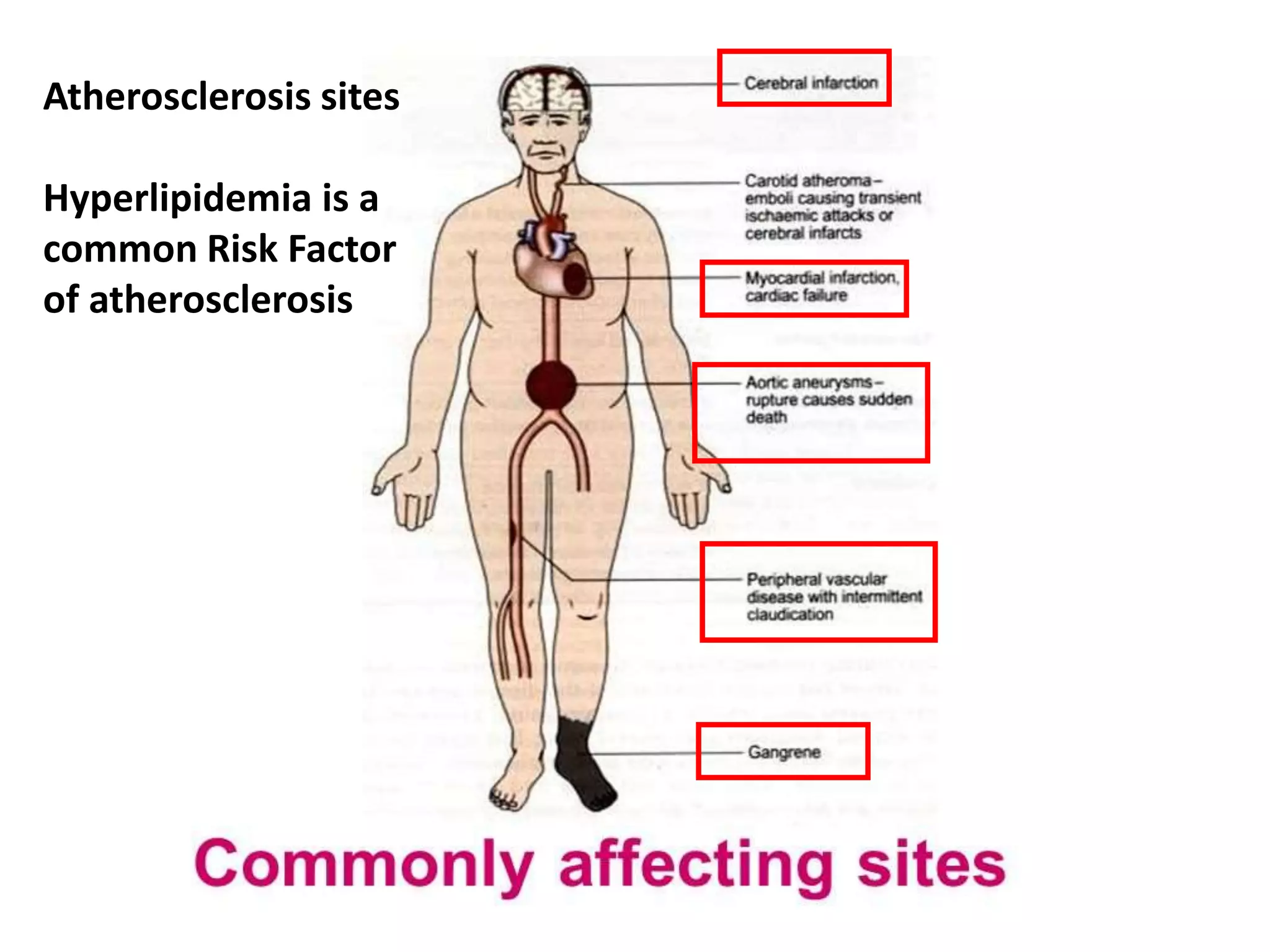
Dyslipidemia, or abnormal lipid levels in the blood, increases the risk of atherosclerosis and cardiovascular disease. The document discusses the definition and causes of dyslipidemia as well as screening recommendations. It also summarizes the roles of different lipids like LDL, HDL, and triglycerides in atherosclerosis. The treatment approaches for different lipid abnormalities are outlined, including lifestyle modifications and medications like statins, fibrates, bile acid sequestrants, nicotinic acid, and ezetimibe.































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



