Downloaded 80 times
![DEFINITION
Dry eye syndrome is a multifactorial disease
of the tears and ocular surface that results in
symptoms of discomfort, visual disturbance, tear
film instability and potential damage to the ocular
surface. It is accompanied by increased osmolarity
of the tear film and inflammation of the ocular
surface.
The ocular surface, 2007, pp. 77. 2007 Report of the International Dry Eye
Workshop (DEWS). [Online] Tear Film and Ocular Surface Society. Available
at www.tearfilm.org/dewsreport](https://image.slidesharecdn.com/101-161026102041/85/Dry-Eyes-2-320.jpg)
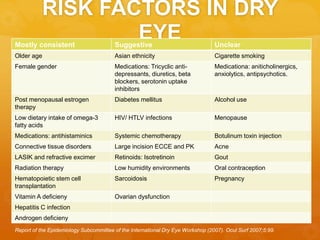
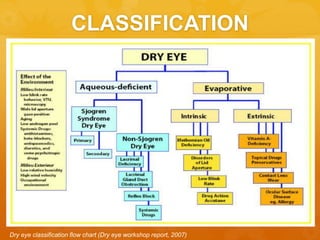
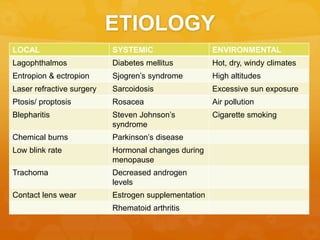

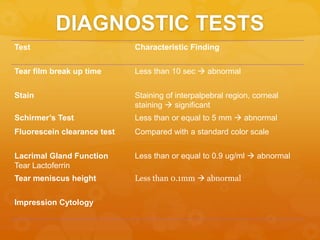
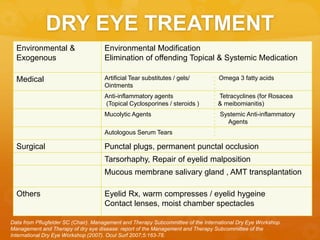

Dry eye syndrome is a multifactorial condition characterized by discomfort, visual disturbances, and potential damage to the ocular surface due to tear film instability and inflammation. Risk factors include older age, certain medications, hormonal changes, and environmental conditions. Diagnosis involves various tests such as tear film break-up time and Schirmer’s test, with treatment options ranging from environmental modifications to medical and surgical interventions.





















































![Dry_Eye_Presentation_Final[1].pptx......](https://cdn.slidesharecdn.com/ss_thumbnails/dryeyepresentationfinal1-250516163834-f963ff70-thumbnail.jpg?width=640&height=640&fit=bounds)




















































