Lipid layer
Outermost superficialoily layer,
Secreted by meibomian gland, Zeiss and Moll glands.
Role :
• prevents rapid tear evaporation
• smoothes the tear film surface, reducing glare and
improving vision
• Acts as barrier for preventing contamination of tear film
4.
Aqueous layer
Middle layer,comprises 60% of the tear film
Secreted by lacrimal gland and the accessory glands
of Krause and wolfring
Contains ions of inorganic salts ,glucose , urea and
various biopolymers such as enzymes , proteins and
glycoproteins
Lysozyme , lactoferrin, tear specific prealbumin and
secretory IgA are main constituents of protein
fraction.
5.
Functions
• Serves toprovide atmospheric oxygen to the
epithelium
• washes away all the debris and noxious irritants and
contains antibacterial substances like lysozymes and
betalysin
6.
Mucin layers
• Secretedby conjunctival goblets cells
• Role :
• Lubricates the ocular and palpebral surfaces
• Provides slippery coating over foreign bodies,thereby
protecting cornea and conjunctiva .
7.
Functions of TearFilm
• Provides a smooth optical surface for clear vision.
• Maintains hydration and protects the corneal
epithelium.
• Acts as a barrier against infections.
• Removes debris and distributes oxygen to the cornea.
8.
8
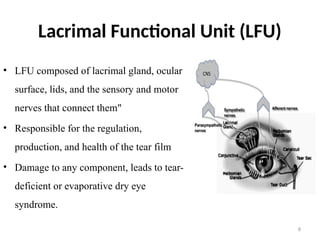
Lacrimal Functional Unit(LFU)
• LFU composed of lacrimal gland, ocular
surface, lids, and the sensory and motor
nerves that connect them"
• Responsible for the regulation,
production, and health of the tear film
• Damage to any component, leads to tear-
deficient or evaporative dry eye
syndrome.
9.
Introduction to DryEye Disease
• DEWS II Definition: Dry Eye Disease is a multifactorial
disease of the ocular surface characterized by a loss of
homeostasis of the tear film that is accompanied by ocular
symptoms ,in which tear film instability and
hyperosmolarity ,ocular surface inflammation and damage ,
and neurosensory abnormalities play etiological roles.
• • Prevalence: Affects millions globally, particularly among
older adults, women, and those with certain systemic
conditions.
10.
NEI definition
• Dryeye disease is a disorder of the tear film due to
reduced tear production or excessive tear evaporation
which causes damamge to the interpalpebral ocular
surface and is associated with symptoms of ocular
discomfort and or visual symptoms
11.
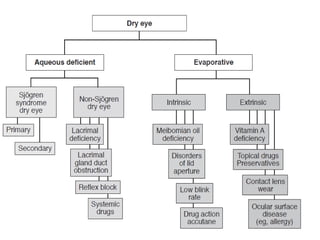
Causes of DryEye Disease
Intrinsic Causes:
• Age: Decreased tear production with aging.
• Hormonal Changes: Particularly in women (e.g.,
menopause).
• Systemic Conditions: Sjogren’s Syndrome,
rheumatoid arthritis, lupus, etc.
• Medications: Antihistamines, antidepressants, blood
pressure medications, etc.
12.
Extrinsic Causes:
• EnvironmentalFactors: Air conditioning, wind,
smoke, and dry climates.
• Contact Lens Wear: Extended use of contact lenses.
• Prolonged Screen Time: Reduced blink rate.
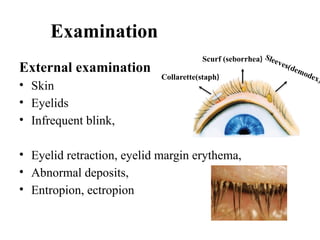
Clinical features
Symptoms
• feelingof dryness, grittiness and burning
• Stringy discharge,
• transient blurring of vision,
• redness and
• crusting of the lids
16.
signs
Posterior (seborrhoeic) blepharitiswith meibomian
gland dysfunction is often present.
Conjunctiva
• Redness.
• Staining with rose Bengal and lissamine green .
• Keratinization.
• Conjunctivochalasis is a common response to, and
exacerbating factor for, the chronic irritation of dry eye,
such that a self-sustaining cycle is maintained.
17.
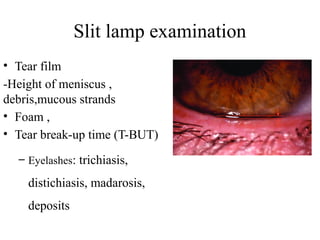
Tear film
• Inthe dry eye, the lipid-contaminated mucin
accumulates in the tear film as particles and debris
that move with each blink
• In the normal eye the meniscus is 0.2–0.4 mm in
height, but in dry eye becomes thin (less than 0.25
mm) or absent
18.
Cornea
• Punctate epithelialerosions that stain well with
fluorescein .
• Filaments consist of strands of mucus and debris
such as shed epithelial cells and are typically attached
at one end to the corneal surface . The filaments stain
well with rose Bengal but less so with fluorescein
Diagnosis of DryEye Disease
•Clinical
History:
Ocular
history
Systemic
history
21.
Ocular history
• Detailedsymptom questions
Ocular surface disease index –OSDI
Dry eye questionnaire -5 (DEQ -5)
Standard patient evaluation of eye dryness questionnaire
(SPEED Q)
National eye institute vision function questionnaire-25
(NEIVFQ)
• Duration and severity of symptoms
• Exacerbating conditions (wind , driving, prolong use of gadgets
like computers , mobile phone )
22.
• patients withaqueous tear deficiency worse as the
day progresses, or after extensive use of the eyes
• Lipid layer deficiency(meibomian gland
disease ,blepharitis) worse in the morning---visual
blurring upon waking
23.
– Topical medicationsused, their frequency and their
effect on symptoms
– Contact lens wear, schedule and care
– Allergic conjunctivitis
• Ocular surgery history (prior keratoplasty, cataract surgery,
keratorefractive surgery, Punctal surgery , Eyelid surgery)
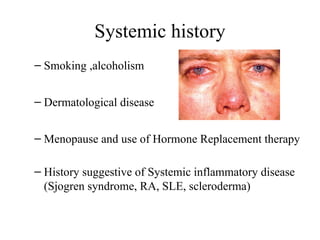
Systemic history
– Smoking,alcoholism
– Dermatological disease
– Menopause and use of Hormone Replacement therapy
– History suggestive of Systemic inflammatory disease
(Sjogren syndrome, RA, SLE, scleroderma)
26.
• Other systemicconditions (lymphoma, sarcoidosis)
• Chronic viral infections (Hep C, HIV)
• Systemic medications
• Trauma (mechanical, chemical, thermal)
• Non-ocular surgery (bone marrow transplant, head
and neck surgery, trigeminal neuralgia surgery)
• Radiation of Head and Neck
• Neurological conditions
27.
Medical history
• Drugs
oralcontraceptives,
anticholinergics,
antihistamines,
antiarrhythmics, Beta blockers
antipsychotics, TCA ,SSRIs
antispasmodics,
diuretics,
retinoids,
chemotherapy.
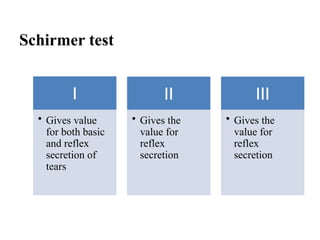
Schirmer test
I
• Givesvalue
for both basic
and reflex
secretion of
tears
II
• Gives the
value for
reflex
secretion
III
• Gives the
value for
reflex
secretion
37.
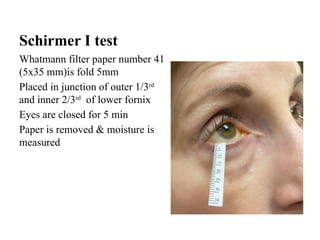
Schirmer I test
Whatmannfilter paper number 41
(5х35 mm)is fold 5mm
Placed in junction of outer 1/3rd
and inner 2/3rd
of lower fornix
Eyes are closed for 5 min
Paper is removed & moisture is
measured
38.
• Schirmer score(mm/5 min)
• Mild –variable
• ≤ 10 – moderate
• ≤ 5- severe
• ≤2 – very severe
39.
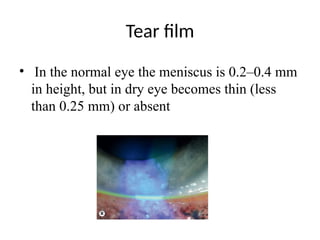
Tear film
• Inthe normal eye the meniscus is 0.2–0.4 mm
in height, but in dry eye becomes thin (less
than 0.25 mm) or absent
40.
40
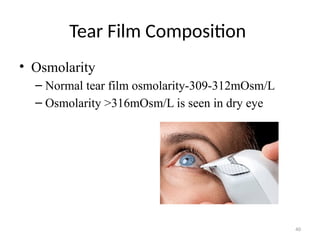
Tear Film Composition
•Osmolarity
– Normal tear film osmolarity-309-312mOsm/L
– Osmolarity >316mOsm/L is seen in dry eye
41.
41
• Tear proteinanalysis:
– May be quantified by measuring tear lysozymes, tear
lactoferrin, epidermal growth factor,
immunoglobulin A
– Lysozyme accounts for 20-40% of total tear protein
– Sensitive but lacks specificity
– Done by spectrophotometry
– Tear lactoferrin concentrations measured by
Lactocard, ELISA technique
Tear film breakup time
Two types
• Invasive
• Non invasive
Keratometer
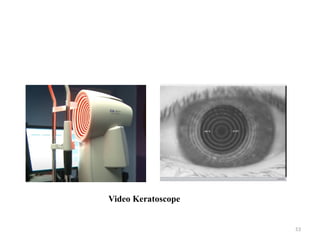
Video keratoscope
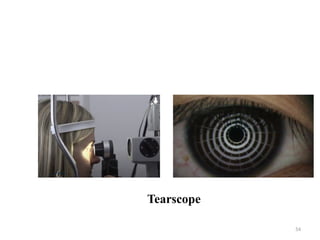
Tearscope
50.
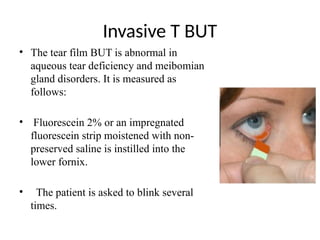
Invasive T BUT
•The tear film BUT is abnormal in
aqueous tear deficiency and meibomian
gland disorders. It is measured as
follows:
• Fluorescein 2% or an impregnated
fluorescein strip moistened with non-
preserved saline is instilled into the
lower fornix.
• The patient is asked to blink several
times.
51.
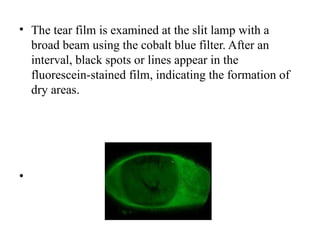
• The tearfilm is examined at the slit lamp with a
broad beam using the cobalt blue filter. After an
interval, black spots or lines appear in the
fluorescein-stained film, indicating the formation of
dry areas.
•
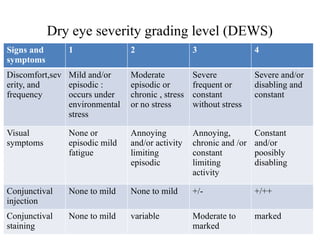
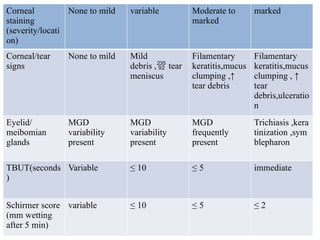
Dry eye severitygrading level (DEWS)
Signs and
symptoms
1 2 3 4
Discomfort,sev
erity, and
frequency
Mild and/or
episodic :
occurs under
environmental
stress
Moderate
episodic or
chronic , stress
or no stress
Severe
frequent or
constant
without stress
Severe and/or
disabling and
constant
Visual
symptoms
None or
episodic mild
fatigue
Annoying
and/or activity
limiting
episodic
Annoying,
chronic and /or
constant
limiting
activity
Constant
and/or
poosibly
disabling
Conjunctival
injection
None to mild None to mild +/- +/++
Conjunctival
staining
None to mild variable Moderate to
marked
marked
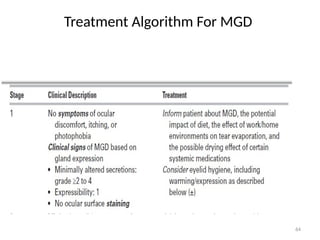
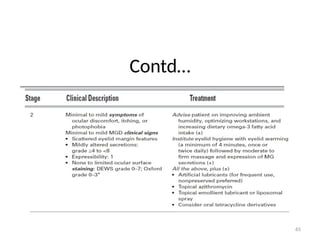
Management of dryeye disease
Level 1 •
Education and environmental/dietary modifications
• Establishment of realistic expectations and emphasis on the
importance of compliance.
• Lifestyle review including the importance of blinking whilst
reading, watching television or using a computer screen and
the management of contact lens wear.
• Environmental review, e.g. increasing humidity may be
possible for some environments.
74.
• Instillation aidsfor eye drops
• Caution the patient that laser refractive surgery can
exacerbate dry eye.
Systemic medication review to exclude contributory
effects and eliminate offending agents.
Discontinuation of toxic/ preserved topical
medication if possible
75.
Artificial tear substitutesincluding gels and
ointments .
Eyelid therapy. warm compresses and lid hygiene for
blepharitis.
Reparative lid surgery (e.g. entropion, ectropion,
excessive lid laxity or scleral show).
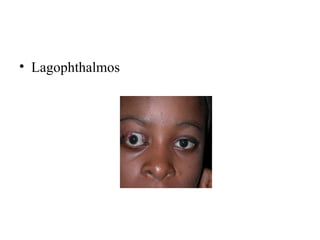
Nocturnal lagophthalmos can be addressed by taping the
lids closed at bedtime, wearing swimming goggles during
sleep, or in extreme cases by lateral tarsorrhaphy
76.
Level 2
Non-preservedtear substitutes
Anti-inflammatory agents such as topical steroids, oral
omega fatty acids and other agents such as topical
ciclosporin.
Tetracyclines (for meibomianitis, rosacea).
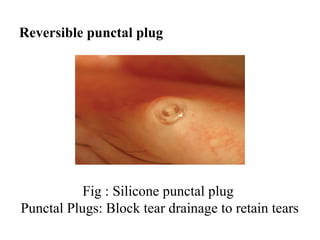
Punctal plugs.
Secretagogues, e.g. pilocarpine, cevimeline, rebamipide.
Moisture chamber spectacles and spectacle side shields.
Surgery
• Eyelid surgery,such as tarsorrhaphy , entropion
correction, ectropion correction , lagophthalmos
correction to decrease tear evaporation.
• Salivary gland auto-transplantation.
• Mucous membrane or amniotic membrane
transplantation for corneal complications
81.
Other potential approaches
•Recombinant human nerve growth factor
(RHNGF) : topical e.coli-derived RHNGF for
treatment of stage 2 and 3 neurotrophic keratitis.
• Bandage soft contact lens : effective in preventing
recurrence of filamentary keratopathy.
• Secretagogues : pilocarpine , cevimeline approved by
FDA to treat symptoms of DRY mouth in patients with
SJS syndrome
Conclusion
• Dry eyedisease is common, multifactorial,
and impactful.
• Early diagnosis and treatment can
significantly improve symptoms.
• Ongoing research shows promise for severe or
refractory cases.
84.
Bibliography
• AAO section8 External diease and cornea
• Kanski’s Clinical Ophthalmology, 10th
Edition
• Parson’s disease of the eye 23rd
edition
• Albert and jokobiec’s principles and practice
of ophthalmology 4th
edition
• Dry Eye Workshop PDF-2007/2017
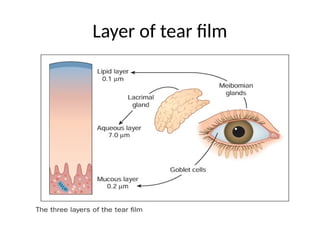
#3 Lipid layers is forms from polar and neutral lipids
#4 Surface tensions of normal aqueous tears=40 and 42 dyn/cm
#8 Regulation of tear film components • Hormonal ○ Androgens are the prime hormones responsible for regu lation of lipid production. ○ Oestrogens and progesterone receptors in the conjunctiva and the lacrimal glands are essential for the normal func tion of these tissues. • Neural via fibres adjacent to the lacrimal glands and goblet cells that stimulate aqueous and mucus secretion.
#13 Primary=occurs in the absence of rheumatic disorder
Secondary=associated with underlying rheumatic disease
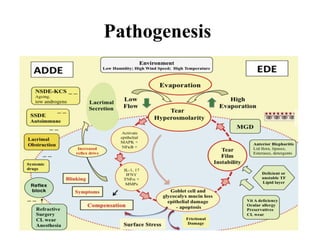
#14 Inflammatory mediators in dry eye. ADDE = aqueous deficient dry eye; CL = contact
the vicious circle. Hyperosmolarity at the ocular surface initiates an inflammatory sequence leading to damage of epithelial cells, goblet cells, punctate epitheliopathy and tear film instability and breakup. Described by the TFOS DEWS II as a “vicious circle” of inflammation, this process is the common final pathway for all forms of DED.
lens; EDE = evaporative dry eye; IFN- γ = interferon gamma; IL-1, 17 = interleukins 1 and 17;
KCS = keratoconjunctivitis sicca; MAPK = mitogen- activated protein kinase; MGD = meibomian
gland dysfunction; MMPs = matrix metalloproteinases; NFκB = nuclear factor kappa- light- chain
enhancer of activated B cells; NSDE = Non- Sjögren dry eye; SSDE = Sjögren syndrome dry eye;
TNF-α = tumor necrosis factor alpha; TF = tear film. (Modified with permission from Craig JP, Nelson JD,
Azar DT, et al. TFOS DEWS II Report executive summary. Ocul Surf. 2017;15(4):802–812. With permission from Elsevier.)
#17 In the normal eye, as the tear film breaks down, the mucin layer becomes contaminated with lipid but is washed away
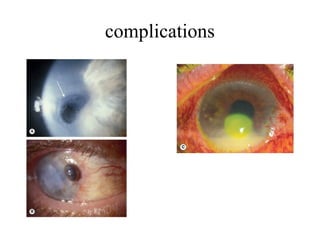
#19 Severe corneal complications of dry eye. (A) Melting (arrow); (B) perforation with iris plugging; (C) bacterial infection
#20 he OSDI, which was created by the Outcomes Research Group at Allergan Inc in order to quickly assess the symptoms of ocular irritation in dry eye disease and how they affect functioning related to vision.[5] This 12-item questionnaire assesses dry eye symptoms and the effects it has on vision-related function in the past week of the patient’s life.[6] The questionnaire has 3 subscales: ocular symptoms, vision-related function, and environmental triggers. Patients rate their responses on a 0 to 4 scale with 0 corresponding to “none of the time” and 4 corresponding to “all of the time.” A final score is calculated which ranges from 0 to 100 with scores 0 to 12 representing normal, 13 to 22 representing mild dry eye disease, 23 to 32 representing moderate dry eye disease, and greater than 33 representing severe dry eye disease.
#21 Tear film n ocular surface society Dry eye workshop II recommends 2 questionnaire
#22 Combination: Evaporative and aqueous deficiency often occur together. May also include a mucin layer tear deficiency.
EYELID REMAINS CLOSED FOR A PROLONGED PERIOD OF TIME DURING SLEEP AND IT ALLOWS EXCESS OIL AND DEBRIS TO ACCUMULATE AROUND EYELASHES---BACTERIAL OVERGROWTH
#23 Likely secondary to disruption of corneal nerves and interference with normal reflex tearing
#25 Image :facial rosacea
Image 2 :stromal keratitis a/w rosacea of face,neck,shoulders
Rosacea is a/w cutaneous sebaceous gland dysfunction
Alcohol consumption can contribute to worsening of facial redness because of its effect on vasomotor stability with dilatation of vessels
rosacea, psoriasis, atopy)
4. Dry mouth, dental cavities and oral ulcer
Smoking irritate eyes.with blinking eyelids coat eye with aprotective layer—keeps dust and debris out—chemicals in smoke can cause this layer to break down.
Smoke is a drying agent that promotes tear evaporation
rosacea, psoriasis, atopy)
4. Dry mouth, dental cavities and oral ulcer
rosacea, psoriasis, atopy)
4. Dry mouth, dental cavities and oral ulcer
(rosacea, psoriasis, atopy)
4. Dry mouth, dental cavities and oral ulcer
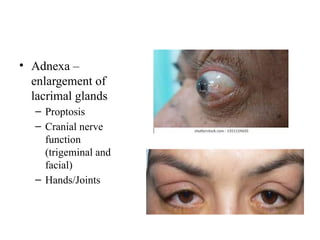
#26 Infiltration of the lacrimal glands (e.g., sarcoidosis, tumor)
Postradiation fibrosis of the lacrimal glands.
#28 Fig1 :illustration showing the clinical signs of blepharitis
Fig2 : referred as cylindrical dandruff,typical of demodicosis
Eyelid scale=scurf
Eyelid cylindrical dandruff=sleeves
Collaretes=fibrinoius scales and matted,flatte ned crusts surrounding individual cilia
Demodex=mites (oral ivermectin,treatment with hypochlorous acid)
blepharitis in staph &seborrheic are located in anterior eyelid margin while in MGD is in posterior eyelid margin
#37 Quantitative test
BASAL SECRETION WHEN CONJUNCTIVA IS ANAESTHESIZED
When measured withput anasthetic it measures basic + reflex secretion
Less than 10 mm of wetting after 5 minutes without anaes thesia or less than 6 mm with anaesthesia is considered abnormal.
PERFORMING TEST IN SIMILAR MANNER
SCHIRMER 2=rubbing unanesthesized nasal mucosa with a dry cotton and noting the wetting after 2 minutes
Schirmer 3 = pt looks directly in the sun ,no diagnostic value and it is potentially dangerous
#39 thin marginal tear meniscus In the normal eye, as the tear film breaks down, the mucin layer becomes contaminated with lipid but is washed away.
In the dry eye, the lipid-contaminated mucin accumulates in the tear film as particles and debris that move with each blink .
The marginal tear meniscus (strip) is a crude measure of the volume of aqueous in the tear film
#40 Although tear osmolarity is sensitive test for identifying dry eye, it lacks specificity . Before doing test makesure pt has not use topical drugs within 2hrs to avoid false osmlarity reading. Test card is inserted in a pen green light ll appear wid a beep sound. Approach pt from side and tears are collected from side with a tip. Successful collection ll be indicated by beep n green light going off,collectd tear fluid ll be assessed using tear lab osmolarity system
#41 Proteins and peptides in tears play an important role in ocular surface disease
Lysozyme analysis is more sensitive but it lacks specificity as it
Tear lactoferrin concentrations measured by Lactocard, commercially available colorimetric solid phase ELISA technique
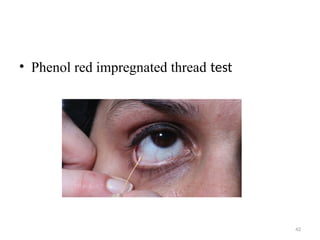
#42 Variation of Schirmer test 75mm long Thread impregnated with phenol red is is kept in lower fornix and reading is taken after 15sec and wetting of thread is noted
9-18mm normal
<6mm abnormal
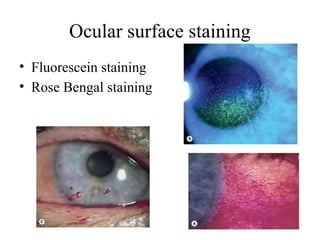
#43 ) Punctate erosions stained with fluorescein;
mild (rose Bengal stain)
Fluorescein stains corneal and conjunctival epithelium (see Fig. 5.6A) where there is sufficient damage to allow the dye to enter the tissues. • Rose Bengal is a dye that has an affinity for dead or devitalized epithelial cells that have a lost or altered mucous layer (Fig. 5.8C). Corneal filaments and plaques (see Fig. 5.6B and D) are also shown up more clearly by the dye and the use of a red-free filter may help visualization. A 1% solution of rose Bengal or a moistened impregnated strip can be used. The dye may cause intense stinging that can last for up to a day, particularly in patients with severe KCS. To minimize irrita tion a very small drop should be used, immediately preceded by a drop of topical anaesthetic and the excess washed out with saline. )
Rose bengal (RB) stains the conjunctiva more intensely than the cornea. The dye stains ocular surface cells that lack a mucouscoating, as well as debris in the tear film [92]. A red-free f ilter makes examination easier. van Bijsterveld developed a scoring system for RB dye that divides the ocular surface into three zones: nasal bulbar conjunctiva, cornea, and temporal bulbar conjunctiva [95]. Each zone is given a score ranging from zero to 3, with zero indicating of breakupoverthecornea. (b) Inahealthysubject, the first breakup is at 13.64 s, and the cornea does notshowareasof breakup no staining and 3 indicating essentially confluent staining. Scores for each eye are totaled according to this system, and scores of 3.5 or greater indicate dry eye.
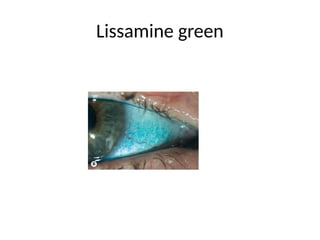
#44 Lissamine green stains in a similar fashion to rose Bengal but causes less irritation and may be preferred
Lissamine green stains dead and degenerated cells and mucus. The staining qual ity of lissamine green is similar to that of RB but is less irritating on the ocular surface.
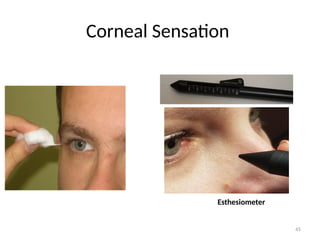
#45 Reduced corneal sensation can be both cause and effect of dry eye Sensory denervation may lead to dry eye by several mechanism:Reducing afferent signal that drives aqueous tear secretion Reducing blink rate There is evidence that corneal sensation decreases secondarily in patient with long standing dry eye. Take cotton swab, extend a few fine strands from tip and gently touch surface of cornea and conjunctiva , patient objective and subjective response can be graded. Apply filament on cornea nd exert slight pressure Cochet bonnet estheiometer shorter the length indicates decreased sensation
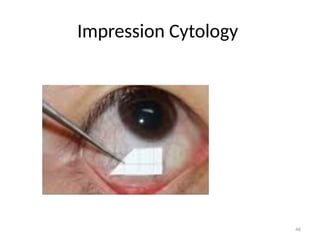
#46 Indication=kcs,atopic keratoconjunctivitis,allergic rhinoconjunctivitis,DES,demonstration of cysts and trophozoites,ocular cicatricical pemphigoid,contact lens wear status,conjunctival squamous metaplasia,ocular surface squamous neoplasia diagnosis and follow up,conjunctival melanosis
Conjunctival impression is taken to examine cellular structure using cellulose acetate filter paper to make impression. Filter paper is cut into small strips and after instillation of topical anesthesia it is pressed against nasal, temporal inferior n superior bulbar conjunctiva with help of forcep, pressure is applied for 2-3 sec, filter paper is then fixed for 10 min in mixuture of 70% ethyl alcohol 37% formaldehyde and glacial acetic acid and examined microscopically. For globlet cell count and keratinization
#47 Useful in screening and evaluating dry eye ,superficial lipid layer is absorbed by tear interferon camera interferon images are then graded on basis of lipid layer stability . Kowa DR-1
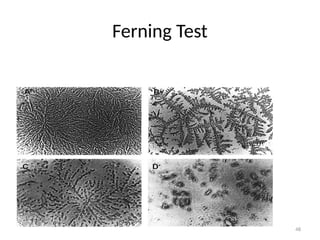
#48 Helps to look quality of tears, 1ul Tear from meniscus is transferred to slide and allowed for evaporation at room temperature and see in a microscope, ferning occurs because of dried mucin
Type 1: uniform large arborization
Type 2: ferning adequate but lesser size
Type 3: partially present, incompletely ferning
Type 4: no ferning
Type 1 and 2 are normal and 3 and 4 are abnormal
#49 Non invasive done by : Tear film stability
Ocular surface health
Tear film composition
Tear flow
Impression cytology
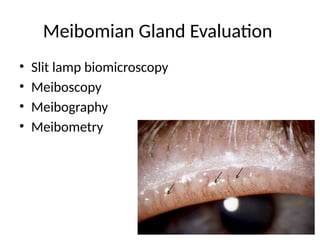
Meibomian gland evaluation
#50 Fluorescein strip is moistened with saline and applied to inferior cul de sac. After several blinks tear film is examined using boroad-beam of slit lamp with blue filter for appearance of first dry spot on ornea.normal is 15-20 sec. value <10 sec indicates tear film instability
Preservative like benzalkonium chloride can artificially speed up tear breakup
#51 The BUT is the interval between the last blink and the appear ance of the first randomly distributed dry spot. A BUT of less than 10 seconds is suspicious.
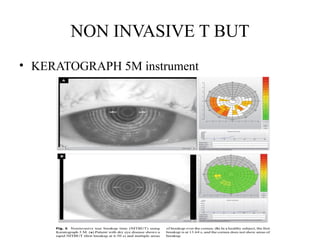
#52 NITBUT is the time (in seconds) it takes for distortions to appear in the image of concentric Placido rings that are reflected on the patient’s cornea by the Keratograph. Two types of NITBUT are measured by the Keratograph 5 M: (i) NITBUT-first is the time at which the first distortion of Placido rings occurs, and (ii) NITBUT-average is the average time of first breakup incidents in different locations in a corneal diameter of 8 mm
#53 Put the pt on video keratoscope ,we can see circular rings on cornea ask pt to blink once n start timer, when circle degrades stop d timer
#55 Meibomian gland is source of lipid in lipid layer of tear film, MGD is most common cause of evaporative dryeye .
Meibomian gland dropout is graded using a 0 to 4 scale based on the area of meibomian gland loss (0, 0%; 1,75%). The score is recorded as “meiboscale” for each eye
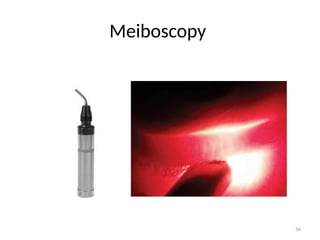
#56 Minimally invasive technique used to assess structure of meibomian glands, meiboscope is transilluminated in upper n lower lid, grand morphology is viewed, no of glands, presence of atrophied gland or dilated gland
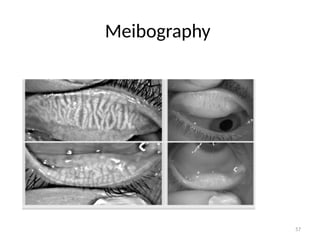
#57 Non invasive method to visualize morphology and density of meibomian glands, using a infrared transilluminator. When infrared coming from transilluinator pass through lipid light becomes scattered, which gives meibomian gland dark apprearane. Normal meiboian gland stripes extend well into depth of eyelid and uniform appearance of gland
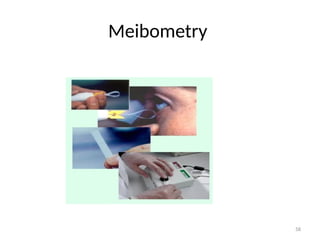
#58 Technique developed to measure basal meibomium level.a sample of meibum at lid margin is transferred to specialized tape whose transparency is altered by exposure to meibum. Degree of change in tape transparency is analyzed photometrically to quantify amt of meibum present in lid margin
#62 Eyelid hygiene is mainstay of treatment. Warm compression:Liquifies thickened secretions softens adherent crustations. Pt should be warned to avoid excessive or uneven heat .application of heat should be followed by Lid massage-express retained secretions Lipid containing artificial tear products are intended to reduce tear evaporation by restoring lipid layer of tear film
#63 Omega-3 fatty acids has been shown to increase average tear production and tear volume. This also block proinflammatory eicosanoid and cytokines
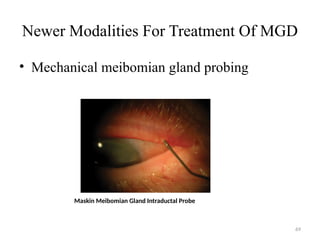
#69 probing using special instruments (Maskin meibomian gland intraductal probe –lyses a fibrovascular membrane growing into duct and may facilitate gland function , permitting normal secretion of meibum
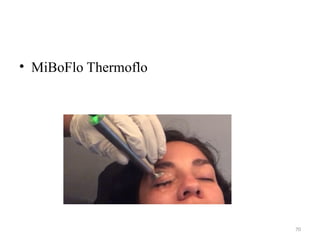
#70 utilizes thermoelectric heat pump to promote liquefaction of meibum
#71 During this procedure, gentle pulses of light are delivered to the skin adjacent to the eyes to reduce inflammation and eliminate any bacterial infection. These pulses melt thick secretions on the eyelids, release the buildup of oil, and unclog the meibomian glands Before beginning the IPL treatment, your doctor will place eye shields over your eyelids to protect them from the bright light pulses. A thin layer of cooling gel will also be applied to the skin around your eyes to protect that sensitive area as well. After the IPL has successfully opened your meibomian glands, your doctor may also express a small amount of oil from the glands in your eyelids to stimulate normal oil flow.
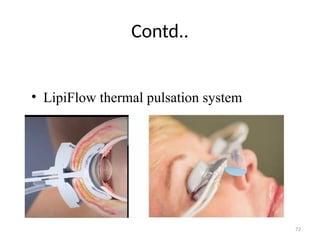
#72 combines gentle pulsatile pressure and thermal energy to increase blood flow to eyelid and open obstructed meiboinian gland ductules, it goes n sits on sclera not touching cornea, post surface sits on inner surface of lower n upper lid
. LipiFlow should not be used in the presence of active infection, postoperatively, or
in the presence of functional abnormalities of the eyelid
#76 In addition to its antibacterial properties, tetracycline inhibits collagenase activ ity [115, 116] and decreases leukocyte chemotaxis and phagocytosis [117, 118]
Pilocarpine at dose of 5mg orally QID is found to be improving patients
low-dose doxycycline (25–50 mg/day) instead of the more common dose of 50–100 mg/day ability to focus their eye during reading and reduced symptoms of blurred vision.
cevelimeCevimeline, another oral cholinergic agonist, may have fewer adverse systemic side effects and be better tolerated than oral pilocarpine due to more selective receptor binding. It also has been found to improve ocular irritation symptoms and aqueous tear production at the 30-mg dose but has not been approved by the FDA for dry eye treatment
Pilocarpine(salagen),cevimeline (evoxac)
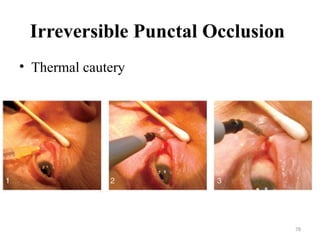
#78 Most cost effective manner of performing irreversible punctal occlusion with a disposable cautery or a radiofrequency probe. Fig1-2% lidocaine is placed 2mm post to punctum to anesthetize plug, tip of cautery device is inserted deep into punctum and horizontal canaliculus. Cautrization is done
#79 Autologous serum tears have been reported to improve ocular irritation symptoms and conjunc tival and corneal dye staining in patients with Sjögren’s syndrome
serum also con tains a variety of growth factors, it can also be useful in neurotrophic dry eye.
Blood-derived eye drop
Contains:
Proteins
Epidermal growth factors
Vitamin A and C
Antioxidants and electrolytes
Mechanism of action of autologous serum eye drops: mimic biochemical properties of natural basal tears in order to heal ocular surface epithelium
#80 A smaller palpebral fissure width decreases the evaporative stress on the tear film and ocular surface
#81 Topical Escherichia coli-derived recombinant human nerve growth factor (RHNGF) has recently been approved by the FDA
Oral medications such as cholinergic agonists, pilocarpine (Salagen), and cevimeline (Evoxac
Pilocarpine, at a dose of 5 mg orally four times a day, improved patients’ ability to focus their eyes during reading and reduced symptoms of blurred vision compared to placebo-treated patients
. Cevimeline, another oral cholinergic agonist, may have fewer adverse systemic side effects and be better tolerated than oral pilocarpine due to more selective receptor binding
Tears contain essential fatty acids, both omega-3 and omega-6, which are not manufactured by the body and only obtained through diet