Downloaded 28 times







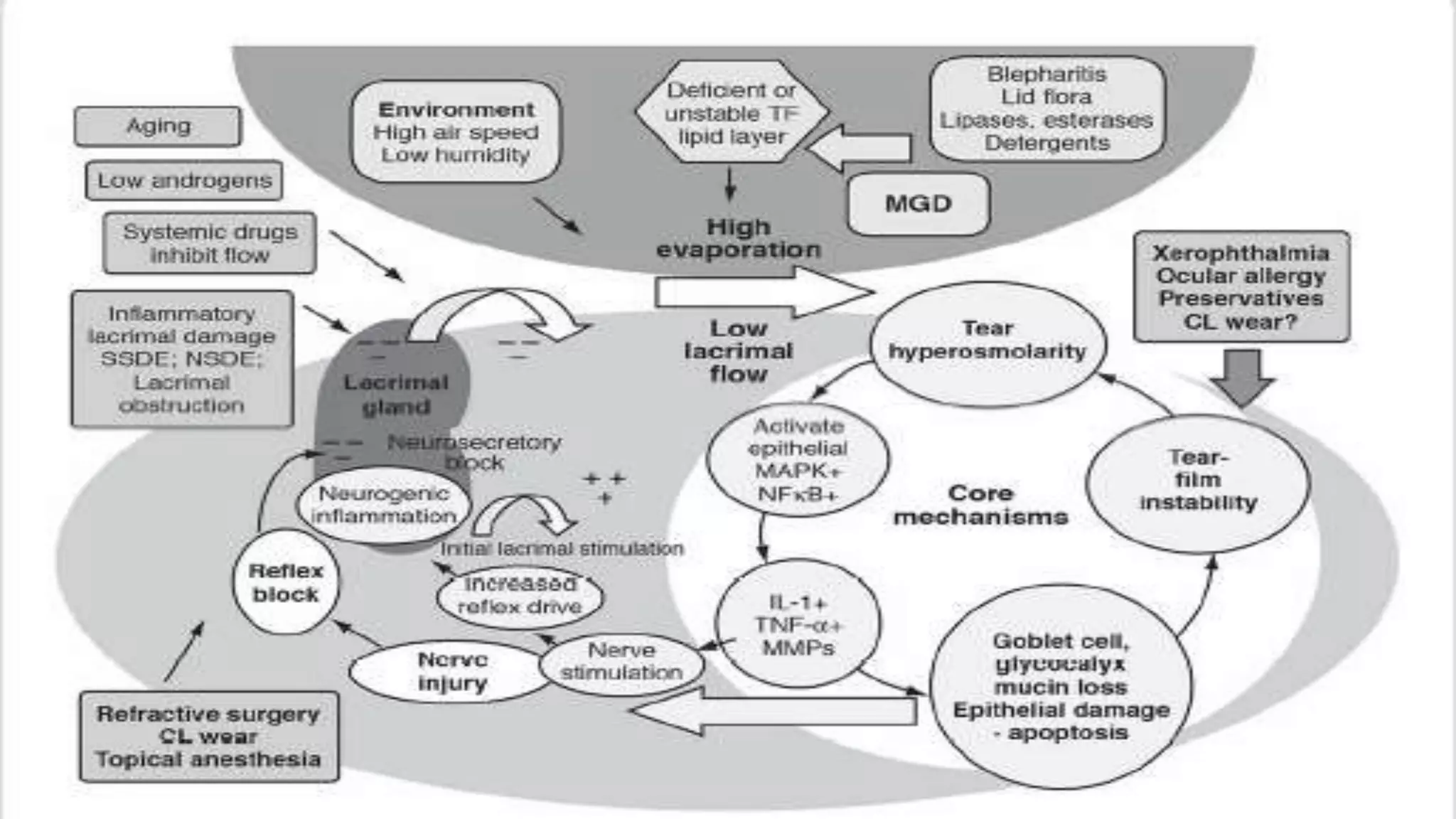
















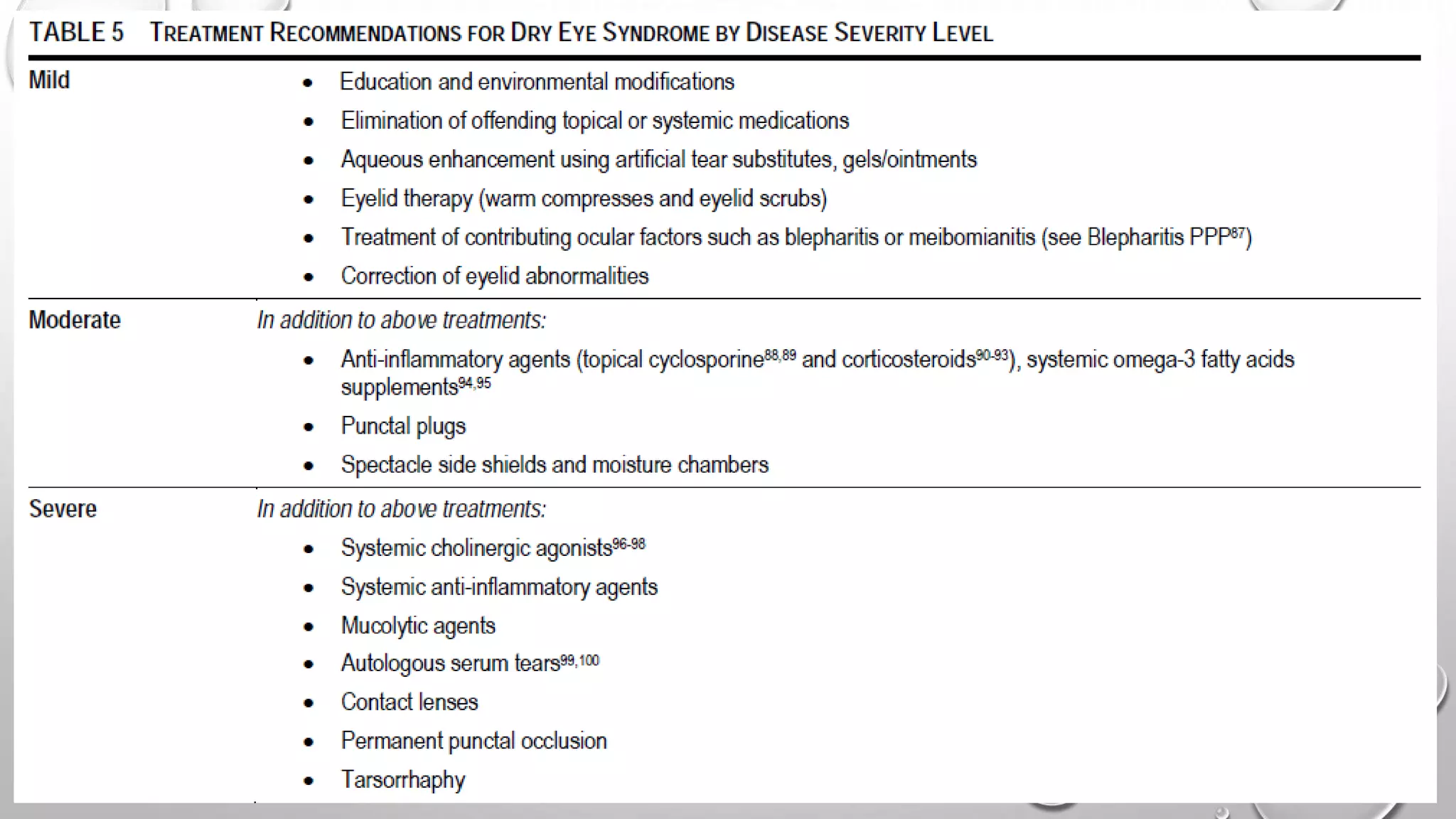
Dry eye syndrome is a highly prevalent disease characterized by loss of tear film homeostasis. It can be classified as aqueous-deficient or evaporative dry eye. Aqueous-deficient dry eye includes Sjögren's syndrome dry eye and non-Sjögren's syndrome dry eye. The pathophysiology involves tear hyperosmolarity, tear film instability, and inflammation of the ocular surface. Diagnosis is based on patient history, examination findings, tear break-up time, ocular surface staining, and tear secretion tests. Treatment depends on disease severity and may include artificial tears, anti-inflammatory medications, punctal plugs, and secretagogues.




































![Dry_Eye_Presentation_Final[1].pptx......](https://cdn.slidesharecdn.com/ss_thumbnails/dryeyepresentationfinal1-250516163834-f963ff70-thumbnail.jpg?width=640&height=640&fit=bounds)






























