Downloaded 21 times







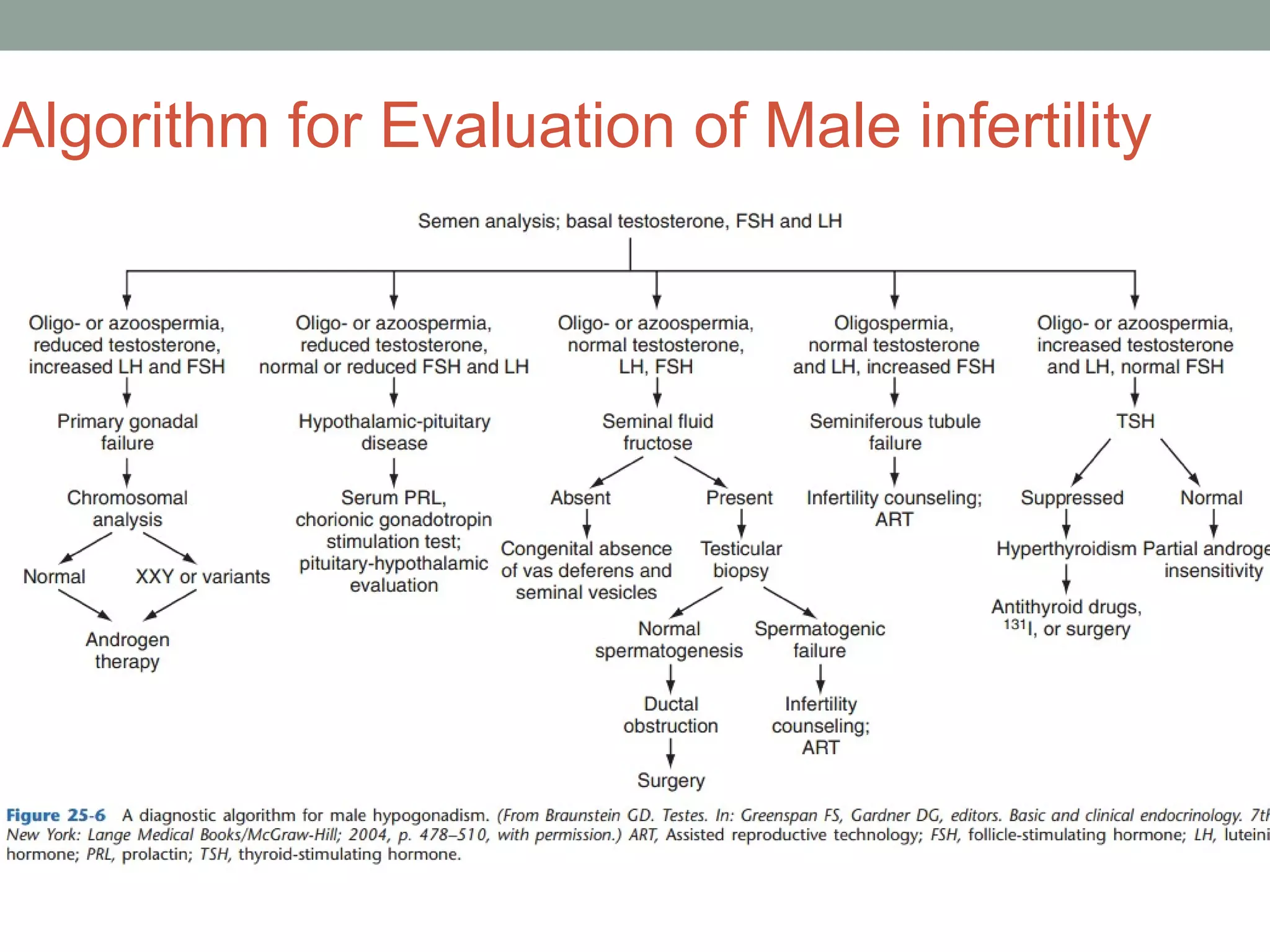




The document discusses various biochemical tests used to evaluate male infertility, including semen analysis to examine sperm count, motility, and morphology, hormone analysis of testosterone, FSH, and LH levels, and immunological tests for sperm antibodies. Abnormalities in these tests can indicate issues like hypogonadism, where low testosterone with high or low FSH indicates testicular or pituitary/hypothalamic dysfunction impairing the hypothalamus-pituitary-testicular axis. A full evaluation including these tests is needed to properly diagnose the underlying cause of infertility in men.






















































































