This document provides information about the hypothalamus including its location, functions, imaging, diseases, and effects of dysfunction. Key points include:
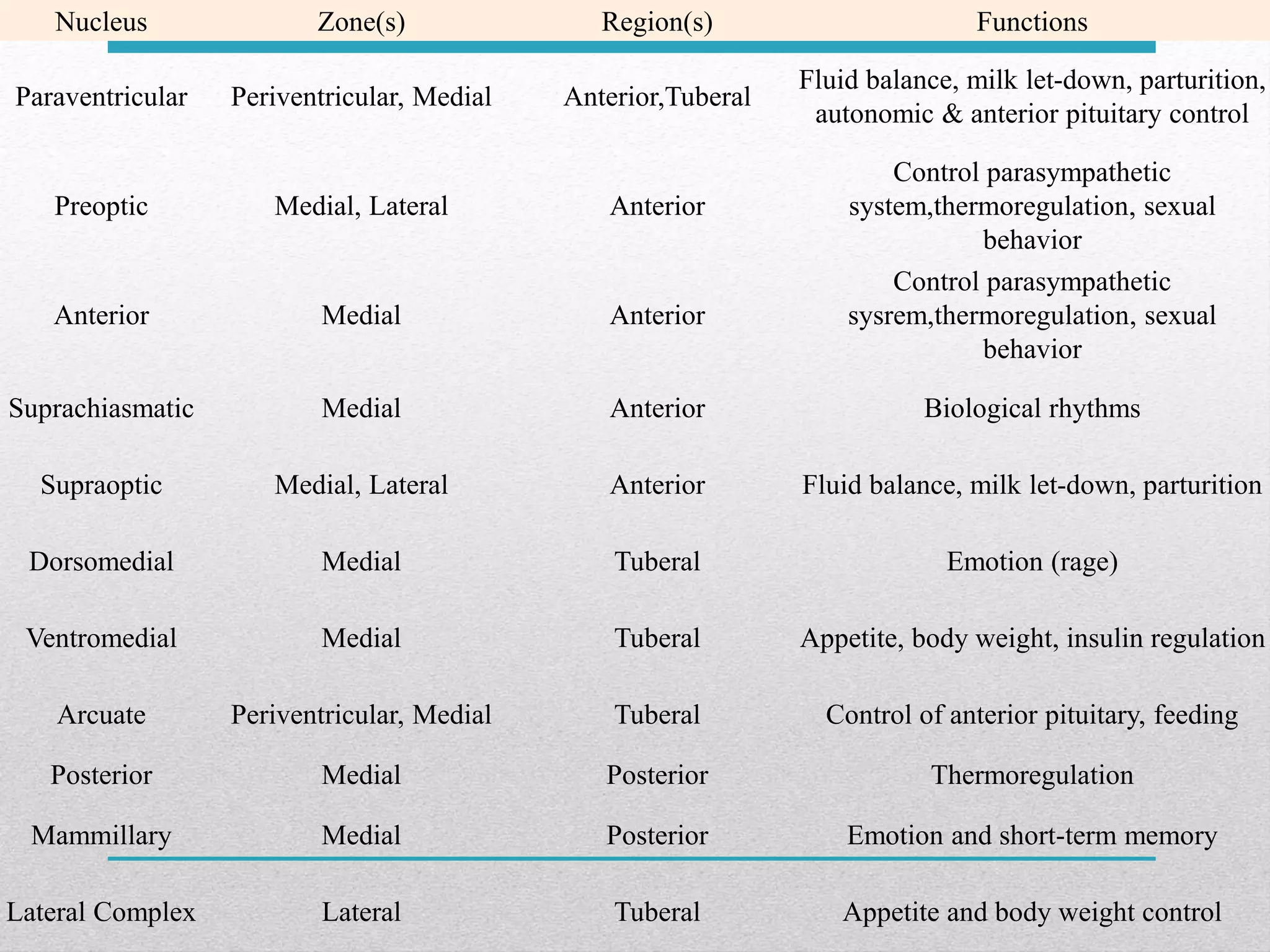
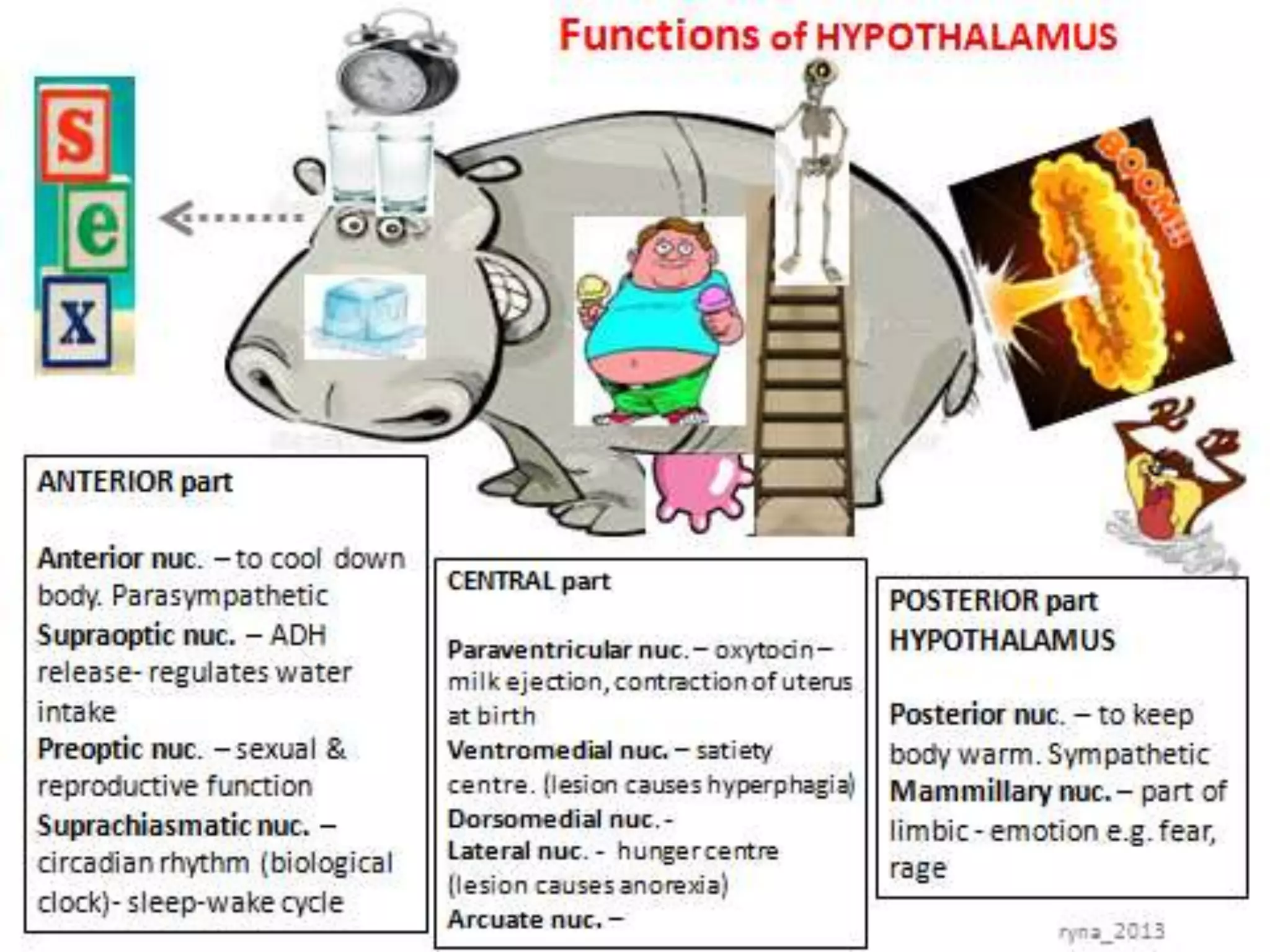
- The hypothalamus is a small region at the base of the brain that controls homeostasis and regulates functions like fluid balance, temperature, hunger, and circadian rhythms.
- MRI is commonly used to image the hypothalamus. Conditions like craniopharyngioma, tuberculosis, sarcoidosis, and strokes can cause hypothalamic diseases or lesions.
- Dysfunction of the hypothalamus can result in endocrine disorders, autonomic dysregulation, temperature dysregulation, and disturbances in appetite/weight control. Prec
















































![A 61-year-old woman developed a rapidly progressive dementia
associated with visual loss. In 7 mo she was dependent for self-care.
Coronal T2-weighted [A], axial FLAIR [B], and axial contrast-enhanced
T1-weighted images [C and D] demonstrate extensive involvement of the
hypothalamic and suprasellar regions, extending laterally towards the optic
tracts, and to the left temporal lobe. The enhancing portion of the lesion is
hypothalamic and suprasellar, and there is also a component of
enhancement in the anterior portion of the temporal lobe (arrow in D).
Neurosarcoidosis involving Hypothalamus](https://image.slidesharecdn.com/hypothalamus-3-150609144057-lva1-app6892/75/Disorder-of-Hypothalamus-61-2048.jpg)




























































![HYPOTHALAMIC AND PITUITARY HORMONES [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamicandpituitaryhormonesautosaved-240606131535-7cfeb320-thumbnail.jpg?width=640&height=640&fit=bounds)






























