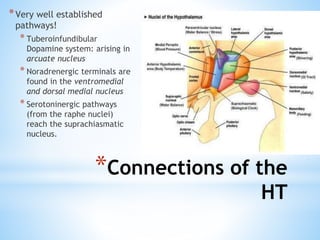
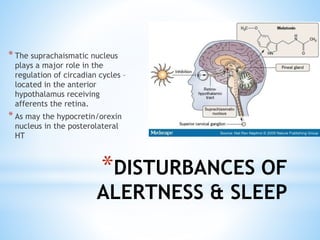
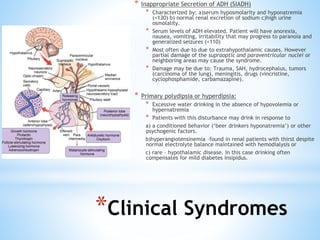
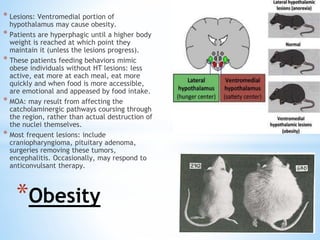
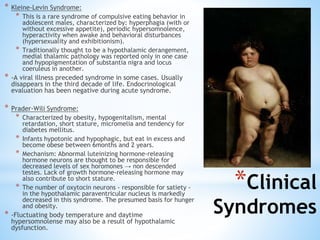
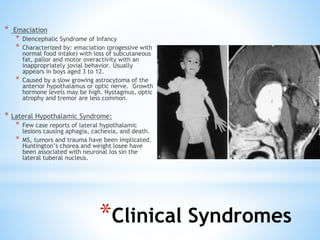
The document discusses various clinical syndromes related to lesions affecting the hypothalamus and pituitary gland. It covers disturbances in temperature regulation like hyperthermia and hypothermia from anterior and posterior hypothalamic lesions. Circadian rhythm abnormalities from suprachiasmatic nucleus lesions and narcolepsy from hypothalamic orexin neuron lesions are described. Autonomic disturbances like cardiac issues, respiratory abnormalities, and gastrointestinal problems are also summarized. Other syndromes covered include diabetes insipidus, inappropriate ADH secretion, obesity, and Kleine-Levin syndrome.