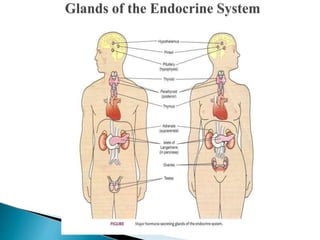
The document discusses endocrine disorders and their causes, including hypofunction and hyperfunction of endocrine glands. It describes the four main types of hormones and provides examples. Signs and symptoms of endocrine disorders are widespread and can include changes in energy, weight, sexual function, mood and sleep. The pituitary gland and its role in controlling other endocrine glands is explained. Common pituitary gland disorders like Cushing's syndrome, acromegaly, and gigantism are summarized. The causes, signs, and treatments of hypopituitarism are covered at a high level. Diabetes insipidus and SIADH, disorders of the posterior pituitary, are defined and their pathophysiology, risks, diagnostic















































![Nephrotic_Syndrome[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nephroticsyndrome1-220824090858-5a841ab2-thumbnail.jpg?width=640&height=640&fit=bounds)




















