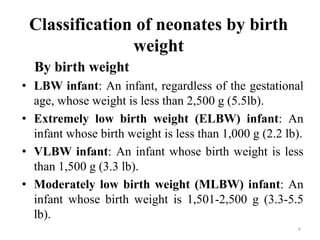
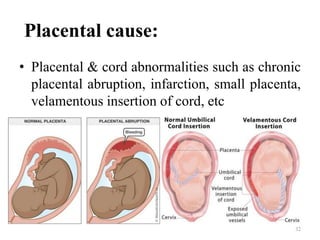
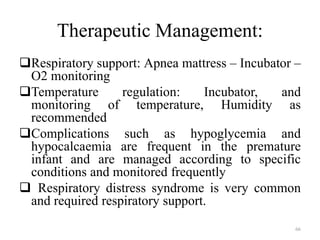
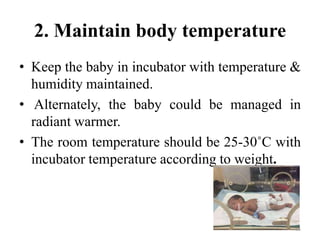
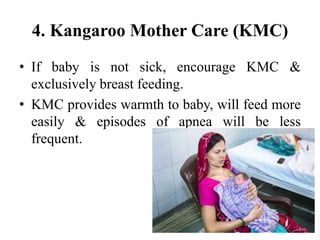
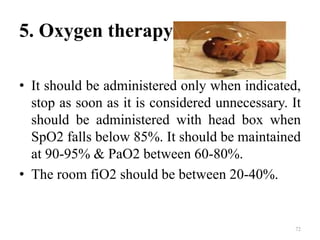
The document discusses low birth weight infants, specifically preterm infants. It defines preterm infants as babies born before 37 weeks of gestation. Preterm infants experience difficulties adapting after birth due to organ system immaturity. Their respiratory, central nervous, circulatory, thermoregulation and gastrointestinal systems are particularly underdeveloped. This can lead to problems like respiratory distress, feeding difficulties, temperature instability, and liver/brain damage. Care of preterm infants focuses on supporting development of these vital functions.






















![Reference :
• Ghai O, Paul V, Bagga A. Ghai Essential Pediatrics. 7th
ed. New delhi, India: CSB; 2012.
• Premature birth - Symptoms and causes [Internet].
Mayo Clinic. 2019 [cited 3 October 2019]. Available
from: https://www.mayoclinic.org/diseases-
conditions/premature-birth/symptoms-causes/syc-
20376730
• Care of the preterm and low-birth-weight newborn
[Internet]. World Health Organization. 2019 [cited 3
October 2019]. Available from:
https://www.who.int/maternal_child_adolescent/newbor
ns/prematurity/en/
91](https://image.slidesharecdn.com/lowbirthweightinfant-final1-220701170109-6be053a3/85/LOW-BIRTH-WEIGHT-INFANT-final-1-pptx-91-320.jpg)