![Definitions
Urinary tract infection
An asymptomatic:
100,000 organisms/ml of urine
Symptomatic:
100 organisms/mL of urine with accompanying
pyuria (>7WBCs]/mL)
Diagnosis should be supported by a positive
culture, particularly with vague symptoms.
Risks:
pyelonephritis,
preterm birth, low birth weight,
increased perinatal mortality.
Aboubakr Elnashar](https://image.slidesharecdn.com/utipregnancy-140803153356-phpapp02/85/Urinary-tract-infections-during-pregnancy-2-320.jpg)

![Renal US is often performed initially, but the
findings are often inconclusive.
A limited IVP (kidneys-ureters-bladder [KUB] with
a 30-min shot after contrast injection) can be
helpful in delineating the site of the obstruction.
Aboubakr Elnashar](https://image.slidesharecdn.com/utipregnancy-140803153356-phpapp02/85/Urinary-tract-infections-during-pregnancy-39-320.jpg)
![Some antibiotics should not be used during
pregnancy:
Tetracyclines (adverse effects on fetal teeth and
bones and congenital defects)
Chloramphenicol (gray syndrome)
Trimethoprim in the first trimester (facial defects
and cardiac abnormalities)
Sulfonamides (hemolytic anemia in mothers with
glucose-6-phosphate dehydrogenase [G6PD]
deficiency, jaundice, and kernicterus) in the third
trimester.
Aboubakr Elnashar](https://image.slidesharecdn.com/utipregnancy-140803153356-phpapp02/85/Urinary-tract-infections-during-pregnancy-58-320.jpg)

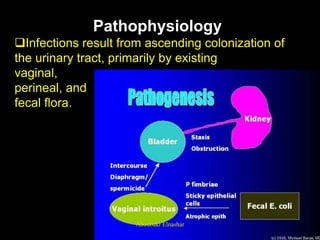
Urinary tract infections during pregnancy can cause complications if left untreated. There are several types of urinary tract infections that can occur, including asymptomatic bacteriuria, acute cystitis, and acute pyelonephritis. Left untreated, these infections have been linked to adverse outcomes like preterm birth and low birth weight. Proper diagnosis involves urine testing and culture. Treatment involves antibiotics, hydration, and pain medications when needed. Screening is important for detecting asymptomatic infections which can later cause issues if not treated.
























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














