Downloaded 58 times
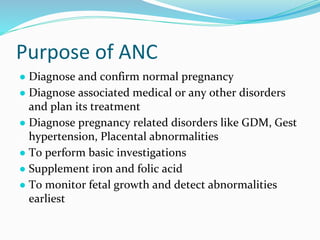
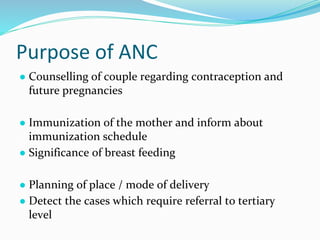


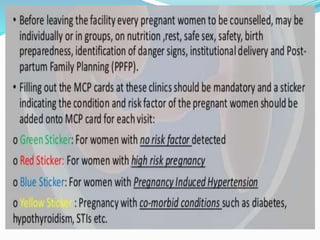
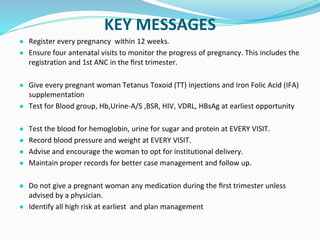

Antenatal care aims to monitor the health of the pregnant woman and fetus through regular checkups. During checkups, healthcare providers take a medical history, conduct examinations, order routine tests, assess risks, provide treatment and advice, and determine the frequency of future visits. The goals are to reduce maternal and infant mortality and morbidity by diagnosing and treating any medical conditions or pregnancy complications early. Key components of antenatal visits include assessing fetal growth, position and heart rate through abdominal examinations. Laboratory tests evaluate anemia and infections. Women are provided iron, folic acid and calcium supplements and immunized. Danger signs that warrant referral to higher facilities include bleeding, decreased fetal movement and high blood pressure.













































































