Table of Contents
Tableof Contents................................................................................................................................................1
A 60-year-old lady presents with sudden-onset diplopia.....................................................................................2
A 50-year-old man presents with sudden-onset horizontal diplopia....................................................................3
A 50-year-old lady complains of vertical diplopia................................................................................................4
A 45-year-old man complains of droopy eyelids that worsen at the end of the day.............................................5
A 45-year-old lady complains of right-sided neck and face pain..........................................................................6
A 30-year-old man presents for a routine eye screening, showing anisocoria worsening in the light with full
extraocular movements......................................................................................................................................7
A young lady complains of painful blurring of vision in the left eye.....................................................................8
A 30-year-old obese lady presents with progressive blurring of vision...............................................................10
A 70-year-old man presents with sudden loss of vision...................................................................................11
A 70-year-old man presents with a 6-month history of painless blurring of vision.............................................12
A 45-year-old lady presents with longstanding blurring of vision......................................................................13
A 25-year-old man presents with poor vision in the right eye since a young age...........................................14
A 45-year-old lady presents with strange-looking discs..................................................................................15
A 70-year-old lady is referred for routine eye screening................................................................................16
A 50-year-old lady complains of difficulty driving...........................................................................................17
A 45-year-old man complains of frequent bumping into objects........................................................................18
2.
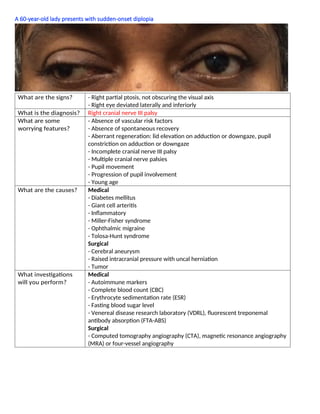
A 60-year-old ladypresents with sudden-onset diplopia
What are the signs? - Right partial ptosis, not obscuring the visual axis
- Right eye deviated laterally and inferiorly
What is the diagnosis? Right cranial nerve III palsy
What are some
worrying features?
- Absence of vascular risk factors
- Absence of spontaneous recovery
- Aberrant regeneration: lid elevation on adduction or downgaze, pupil
constriction on adduction or downgaze
- Incomplete cranial nerve III palsy
- Multiple cranial nerve palsies
- Pupil movement
- Progression of pupil involvement
- Young age
What are the causes? Medical
- Diabetes mellitus
- Giant cell arteritis
- Inflammatory
- Miller-Fisher syndrome
- Ophthalmic migraine
- Tolosa-Hunt syndrome
Surgical
- Cerebral aneurysm
- Raised intracranial pressure with uncal herniation
- Tumor
What investigations
will you perform?
Medical
- Autoimmune markers
- Complete blood count (CBC)
- Erythrocyte sedimentation rate (ESR)
- Fasting blood sugar level
- Venereal disease research laboratory (VDRL), fluorescent treponemal
antibody absorption (FTA-ABS)
Surgical
- Computed tomography angiography (CTA), magnetic resonance angiography
(MRA) or four-vessel angiography
3.
A 50-year-old manpresents with sudden-onset horizontal diplopia
What are the signs? - Right esotropia in primary gaze
- Right abduction deficit
What is the diagnosis? Right sixth nerve palsy
What else do you look
for on examination?
- Extraocular movements (involvement of cranial nerve III)
- Check ability to intort on abduction (failure would suggest involvement of
cranial nerve IV)
- Check pupils (involvement of cranial nerve II)
- Check fundus for papilledema (false localizing sign of raised intracranial
pressure, idiopathic intracranial hypertension)
- Check ears for battle sign (petrous bone fracture)
- Examine neurologically
Contralateral hemiparesis (Raymond's syndrome)
Cranial nerve VII palsy and contralateral hemiparesis (Millard-Gubler
syndrome)
Cranial nerve V, VII and VIII palsy, cerebellar signs (Cerebellopontine angle
tumor - acoustic neuroma)
- Horizontal gaze palsy, cranial nerves V and VII palsy, Horner's syndrome
(Foville's syndrome)
What is the differential
diagnoses?
- Convergence spasm
- Divergence insufficiency
- Duane syndrome
- Longstanding esotropia
- Myasthenia gravis
- Medial wall fracture
- Thyroid eye disease
What are the causes? - Gradenigo syndrome: mastoiditis/petrositis
- Raised intracranial pressure: space occupying lesion, idiopathic intracranial
hypertension
- Tumors: nasopharyngeal carcinoma
- Vascular: ischemia, giant cell arteritis
4.
A 50-year-old ladycomplains of vertical diplopia
What are the signs? - Right hypertropia
- Limitation of downward movement of right eye in down and left gaze
- Over-elevation of the right eye in up and left gaze
What is the diagnosis? Right cranial nerve IV palsy
What Investigations or
examination will you
perform?
- Park's three-step test
- Double Maddox rod test (excyclotorsion)
- Examine old photos (differentiate congenital versus acquired cranial nerve IV
palsy) -Vertical fusional range (increased in congenital cranial nerve IV palsy)
What is the differential
diagnoses?
- Myasthenia gravis
- Orbital fracture
- Partial cranial nerve III palsy
- Skew deviation
- Thyroid eye disease
What are the treatment
options?
- Bangerter foil
- Patching
- Fresnel prism
- Surgery: if stable over six months
5.
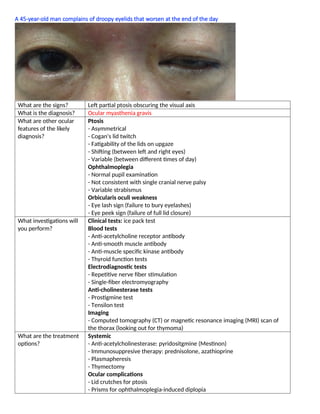
A 45-year-old mancomplains of droopy eyelids that worsen at the end of the day
What are the signs? Left partial ptosis obscuring the visual axis
What is the diagnosis? Ocular myasthenia gravis
What are other ocular
features of the likely
diagnosis?
Ptosis
- Asymmetrical
- Cogan's lid twitch
- Fatigability of the lids on upgaze
- Shifting (between left and right eyes)
- Variable (between different times of day)
Ophthalmoplegia
- Normal pupil examination
- Not consistent with single cranial nerve palsy
- Variable strabismus
Orbicularis oculi weakness
- Eye lash sign (failure to bury eyelashes)
- Eye peek sign (failure of full lid closure)
What investigations will
you perform?
Clinical tests: ice pack test
Blood tests
- Anti-acetylcholine receptor antibody
- Anti-smooth muscle antibody
- Anti-muscle specific kinase antibody
- Thyroid function tests
Electrodiagnostic tests
- Repetitive nerve fiber stimulation
- Single-fiber electromyography
Anti-cholinesterase tests
- Prostigmine test
- Tensilon test
Imaging
- Computed tomography (CT) or magnetic resonance imaging (MRI) scan of
the thorax (looking out for thymoma)
What are the treatment
options?
Systemic
- Anti-acetylcholinesterase: pyridositgmine (Mestinon)
- Immunosuppresive therapy: prednisolone, azathioprine
- Plasmapheresis
- Thymectomy
Ocular complications
- Lid crutches for ptosis
- Prisms for ophthalmoplegia-induced diplopia
6.
A 45-year-old ladycomplains of right-sided neck and face pain
What are the signs? - Anisocoria with the right pupil smaller than the left
- Right partial ptosis (right upper lid lifted up to expose the visual axis)
What is the diagnosis? Right Horner's syndrome
What are the causes? Central (first order)
- Brainstem cerebrovascular accident
- Multiple sclerosis
- Spinal cord tumor
- Trauma
Preganglionic (second order)
- Pancoast tumor
- Subclavian aneurysm
- Thyroid cancer
- Trauma
- Vertebral metastasis
Postganglionic (third order)
- Carotid dissection
- Cluster headache
- Cavernous sinus syndrome
How do you confirm the
diagnosis?
- Apraclonidine 0.5% eye drops (reversal of anisocoria)
- Cocaine 10% (failure to dilate in the Horner's pupil)
How do you localize the
lesion?
- Hydroxyamphetamine 1%
- Phenylephrine 1%
- Decreased sweating over hemi-face of the affected side
What imaging would you
perform?
- Magnetic resonance imaging (MRI) of brain and neck
- Magnetic resonance angiography (MRA)
- Computed tomography (CT) of thorax
What are the causes of
small pupils?
- Horner's syndrome
- Longstanding Adie
- Neurosyphillis (Agryll Robertson)
- Pharmacological
- Uveitis
7.
A 30-year-old manpresents for a routine eye screening, showing anisocoria worsening in the light with full
extraocular movements
What are the signs? Anisocoria with the right pupil larger than the left
What is the most likely
diagnosis?
Tonic pupil
What are other features
of this condition?
- Light near dissociation
- Slow constriction and dilatation of the pupil
- Vermiform movements of the iris (constriction of the iris in segments)
How do you confirm the
diagnosis?
0.125% pilocarpine (constriction of tonic pupil secondary to denervation
hypersensitivity)
Where is the lesion? Ciliary ganglion or short ciliary nerves
What are the causes? Primary
- Holmes-Adie pupil
- Holmes-Adie syndrome (associated with areflexia)
Secondary
- Degenerative
- Diabetes mellitus
- Iatrogenic/trauma
- Myotonia dystrophica
- Parkinson's disease
- Progressive supranuclear palsy
- Syphilis
- Tumor
8.
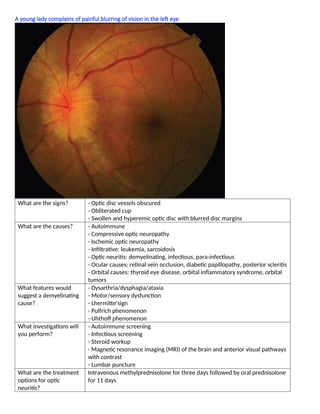
A young ladycomplains of painful blurring of vision in the left eye
What are the signs? - Optic disc vessels obscured
- Obliterated cup
- Swollen and hyperemic optic disc with blurred disc margins
What are the causes? - Autoimmune
- Compressive optic neuropathy
- Ischemic optic neuropathy
- Infiltrative: leukemia, sarcoidosis
- Optic neuritis: demyelinating, infectious, para-infectious
- Ocular causes: retinal vein occlusion, diabetic papillopathy, posterior scleritis
- Orbital causes: thyroid eye disease, orbital inflammatory syndrome, orbital
tumors
What features would
suggest a demyelinating
cause?
- Dysarthria/dysphagia/ataxia
- Motor/sensory dysfunction
- Lhermitte'sign
- Pulfrich phenomenon
- Uhthoff phenomenon
What investigations will
you perform?
- Autoimmune screening
- Infectious screening
- Steroid workup
- Magnetic resonance imaging (MRI) of the brain and anterior visual pathways
with contrast
- Lumbar puncture
What are the treatment
options for optic
neuritis?
Intravenous methylprednisolone for three days followed by oral prednisolone
for 11 days
9.
What are the
complicationsof
steroids?
Ocular
- Cataract, glaucoma, exacerbation of infection (e.g. HSV)
Systemic
- Cardiac: arrhythmia, heart failure
- Ischemic necrosis of the femur
- Malignant hypertension, hyperglycemia, herpetic failure
- Neutropenia, infection: reactivation of tuberculosis
- Psychosis
- Skin changes: hirsutism, acne, moon facies, buffalo hump
- Suppression hypothalamic-pituitary-adrenal axis: shock
- Ulcer: gastric ulcers, bleeding of gastrointestinal tract
10.
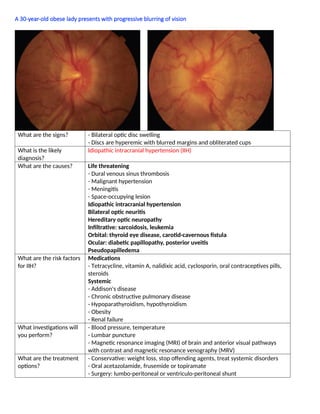
A 30-year-old obeselady presents with progressive blurring of vision
What are the signs? - Bilateral optic disc swelling
- Discs are hyperemic with blurred margins and obliterated cups
What is the likely
diagnosis?
Idiopathic intracranial hypertension (IIH)
What are the causes? Life threatening
- Dural venous sinus thrombosis
- Malignant hypertension
- Meningitis
- Space-occupying lesion
Idiopathic intracranial hypertension
Bilateral optic neuritis
Hereditary optic neuropathy
Infiltrative: sarcoidosis, leukemia
Orbital: thyroid eye disease, carotid-cavernous fistula
Ocular: diabetic papillopathy, posterior uveitis
Pseudopapilledema
What are the risk factors
for IIH?
Medications
- Tetracycline, vitamin A, nalidixic acid, cyclosporin, oral contraceptives pills,
steroids
Systemic
- Addison's disease
- Chronic obstructive pulmonary disease
- Hypoparathyroidism, hypothyroidism
- Obesity
- Renal failure
What investigations will
you perform?
- Blood pressure, temperature
- Lumbar puncture
- Magnetic resonance imaging (MRI) of brain and anterior visual pathways
with contrast and magnetic resonance venography (MRV)
What are the treatment
options?
- Conservative: weight loss, stop offending agents, treat systemic disorders
- Oral acetazolamide, frusemide or topiramate
- Surgery: lumbo-peritoneal or ventriculo-peritoneal shunt
11.
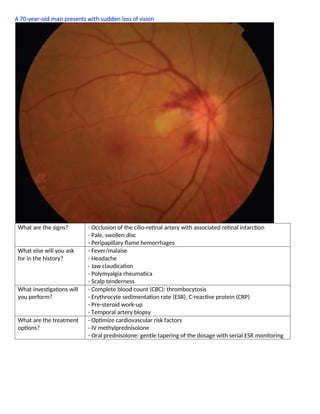
A 70-year-old manpresents with sudden loss of vision
What are the signs? - Occlusion of the cilio-retinal artery with associated retinal infarction
- Pale, swollen disc
- Peripapillary flame hemorrhages
What else will you ask
for in the history?
- Fever/malaise
- Headache
- Jaw claudication
- Polymyalgia rheumatica
- Scalp tenderness
What investigations will
you perform?
- Complete blood count (CBC): thrombocytosis
- Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)
- Pre-steroid work-up
- Temporal artery biopsy
What are the treatment
options?
- Optimize cardiovascular risk factors
- IV methylprednisolone
- Oral prednisolone: gentle tapering of the dosage with serial ESR monitoring
12.
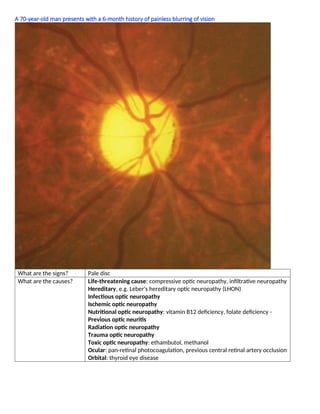
A 70-year-old manpresents with a 6-month history of painless blurring of vision
What are the signs? Pale disc
What are the causes? Life-threatening cause: compressive optic neuropathy, infiltrative neuropathy
Hereditary, e.g. Leber's hereditary optic neuropathy (LHON)
Infectious optic neuropathy
Ischemic optic neuropathy
Nutritional optic neuropathy: vitamin B12 deficiency, folate deficiency -
Previous optic neuritis
Radiation optic neuropathy
Trauma optic neuropathy
Toxic optic neuropathy: ethambutol, methanol
Ocular: pan-retinal photocoagulation, previous central retinal artery occlusion
Orbital: thyroid eye disease
13.
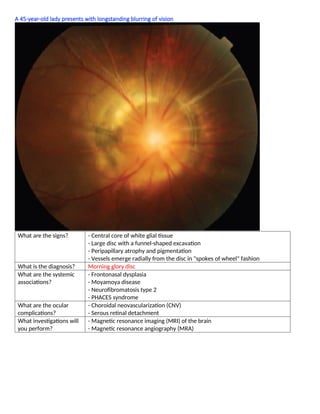
A 45-year-old ladypresents with longstanding blurring of vision
What are the signs? - Central core of white glial tissue
- Large disc with a funnel-shaped excavation
- Peripapillary atrophy and pigmentation
- Vessels emerge radially from the disc in "spokes of wheel" fashion
What is the diagnosis? Morning glory disc
What are the systemic
associations?
- Frontonasal dysplasia
- Moyamoya disease
- Neurofibromatosis type 2
- PHACES syndrome
What are the ocular
complications?
- Choroidal neovascularization (CNV)
- Serous retinal detachment
What investigations will
you perform?
- Magnetic resonance imaging (MRI) of the brain
- Magnetic resonance angiography (MRA)
14.
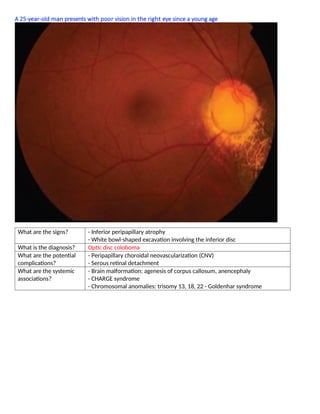
A 25-year-old manpresents with poor vision in the right eye since a young age
What are the signs? - Inferior peripapillary atrophy
- White bowl-shaped excavation involving the inferior disc
What is the diagnosis? Optic disc coloboma
What are the potential
complications?
- Peripapillary choroidal neovascularization (CNV)
- Serous retinal detachment
What are the systemic
associations?
- Brain malformation: agenesis of corpus callosum, anencephaly
- CHARGE syndrome
- Chromosomal anomalies: trisomy 13, 18, 22 - Goldenhar syndrome
15.
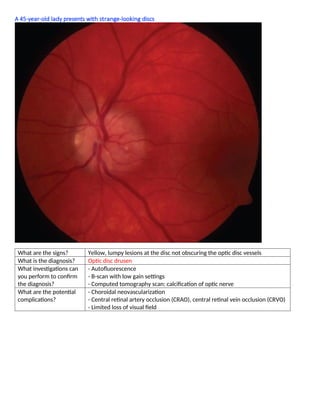
A 45-year-old ladypresents with strange-looking discs
What are the signs? Yellow, lumpy lesions at the disc not obscuring the optic disc vessels
What is the diagnosis? Optic disc drusen
What investigations can
you perform to confirm
the diagnosis?
- Autofluorescence
- B-scan with low gain settings
- Computed tomography scan: calcification of optic nerve
What are the potential
complications?
- Choroidal neovascularization
- Central retinal artery occlusion (CRAO), central retinal vein occlusion (CRVO)
- Limited loss of visual field
16.
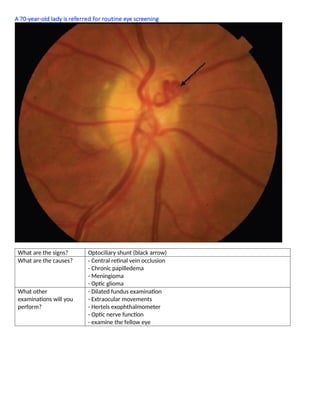
A 70-year-old ladyis referred for routine eye screening
What are the signs? Optociliary shunt (black arrow)
What are the causes? - Central retinal vein occlusion
- Chronic papilledema
- Meningioma
- Optic glioma
What other
examinations will you
perform?
- Dilated fundus examination
- Extraocular movements
- Hertels exophthalmometer
- Optic nerve function
- examine the fellow eye
17.
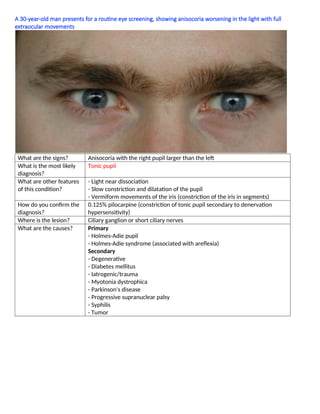
A 50-year-old ladycomplains of difficulty driving
What are the signs? Bitemporal hemianopia respecting the midline
What are the differential
diagnoses?
Infective: tuberculosis
Infiltrative: sarcoidosis
Tumor: pitutary tumor/apoplexy, craniopharyngioma, parasellar meningioma
What investigations will
you perform?
Blood: Hormone level prolactin [others: oxytocin, follicle-stimulating
hormone (FSH), luteinising hormone (LH), thyroid-stimulating hormone (TSH),
adrenocorticotropic hormone (ACTH), growth hormone (GH), antidiuretic
hormone (ADH)]
Magnetic resonance imaging (MRI) of brain and anterior visual pathway with
contrast
What are the treatment
options?
- Co-manage with the endocrinologist to optimize any endocrine dysfunction
- Hormonal therapy: bromocriptine, cabergoline, somatostatin analogues (for
prolactinoma)
- Gamma knife stereotactic radiosurgery
- Surgery: transphenoidal or transethmoidal resection
18.
A 45-year-old mancomplains of frequent bumping into objects
What are the signs? Left superior homonymous quadrantinopia
Where is the lesion? Right retro-chiasmal lesion (likely temporal or inferior occipital lesion)
What investigations will
you perform?
Magnetic resonance imaging (MRI) of brain with contrast
What features would
suggest an occipital
cortex lesion?
- Congruence
- Optokinetic nystagmus (OKN) symmetry
- Unformed visual hallucinations
What are features of a
parietal lobe lesion?
Dominant lobe
- Agraphia
- Acalculia
- Apraxia
- Finger agnosia
- Right-left disorientation
Non-dominant lobe
- Hemi-neglect
- Impaired constructional ability (constructional apraxia)
- Dyscalculia
What are features of a
temporal lobe lesion?
- Auditory hallucination
- dejavú hallucination
- Formed visual hallucination
- Seizures





![A 50-year-old lady complains of difficulty driving
What are the signs? Bitemporal hemianopia respecting the midline
What are the differential
diagnoses?
Infective: tuberculosis
Infiltrative: sarcoidosis
Tumor: pitutary tumor/apoplexy, craniopharyngioma, parasellar meningioma
What investigations will
you perform?
Blood: Hormone level prolactin [others: oxytocin, follicle-stimulating
hormone (FSH), luteinising hormone (LH), thyroid-stimulating hormone (TSH),
adrenocorticotropic hormone (ACTH), growth hormone (GH), antidiuretic
hormone (ADH)]
Magnetic resonance imaging (MRI) of brain and anterior visual pathway with
contrast
What are the treatment
options?
- Co-manage with the endocrinologist to optimize any endocrine dysfunction
- Hormonal therapy: bromocriptine, cabergoline, somatostatin analogues (for
prolactinoma)
- Gamma knife stereotactic radiosurgery
- Surgery: transphenoidal or transethmoidal resection](https://image.slidesharecdn.com/16objectivestructuredclinicalexaminationosceneuro-ophthalmology-250522170846-74b70294/85/16-Objective-Structured-Clinical-Examination-OSCE-Neuro-Ophthalmology-docx-17-320.jpg)
























































































