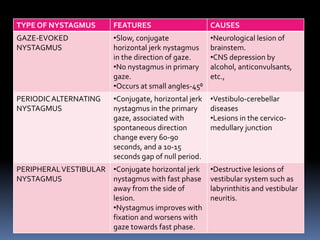
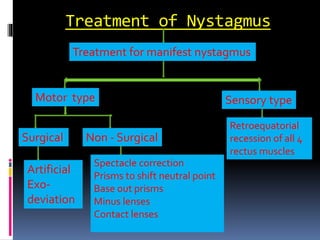
Nystagmus is defined as involuntary oscillatory movements of the eyes and can be classified into various types, including physiological, congenital, and acquired nystagmus. Its etiology involves disturbances in sensory visual pathways and vestibular apparatus, leading to different characteristics such as direction, amplitude, and frequency of the eye movements. Management focuses on improving visual acuity and stabilizing the eyes through optical, medical, and surgical approaches, while also considering the social and educational challenges faced by patients.