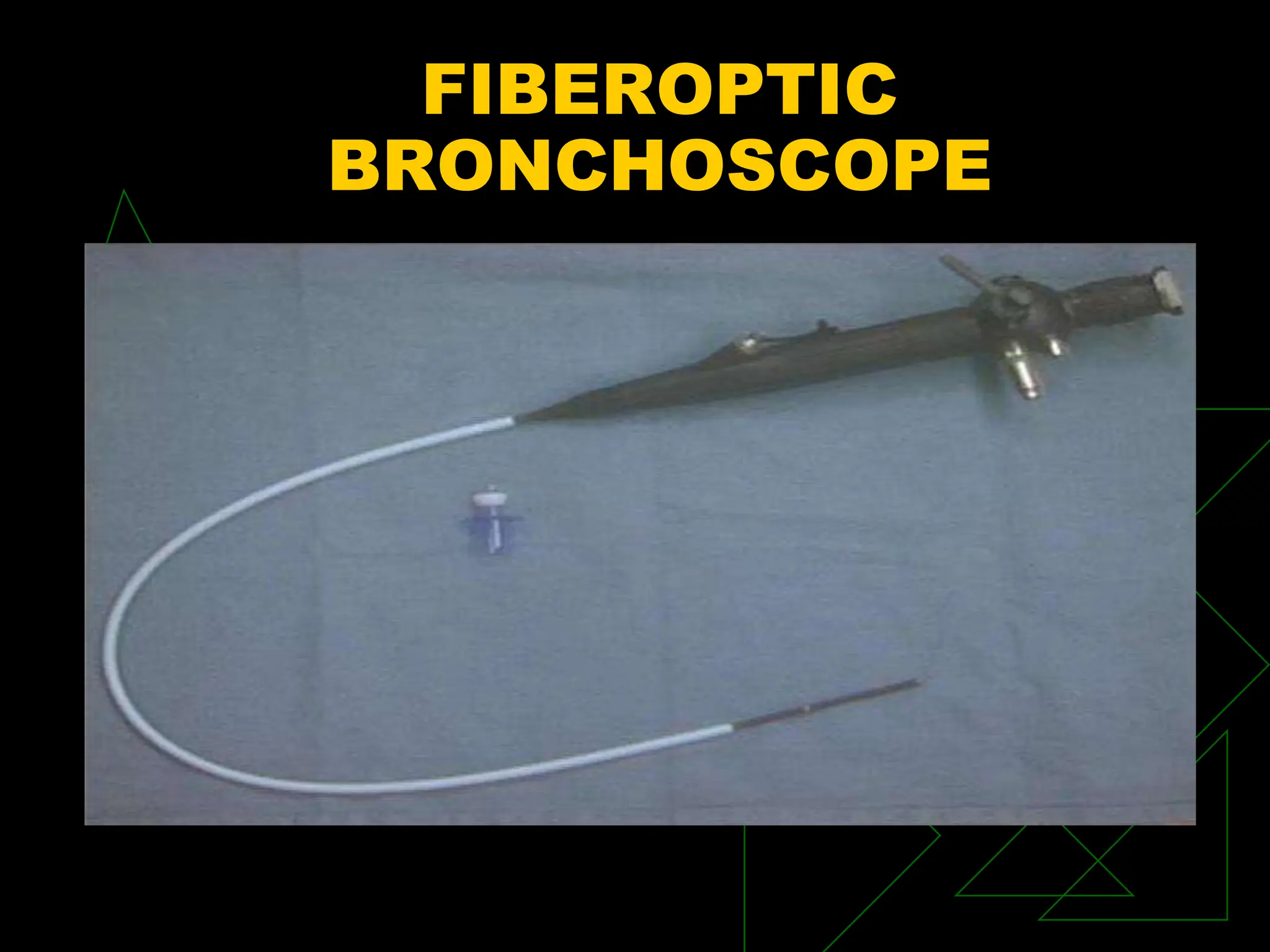
This document discusses various airway management techniques and equipment. It covers indications for intubation, advantages and disadvantages of different airway devices, identification of difficult airways, and equipment for managing difficult airways. Key points include types of endotracheal tubes, methods for confirming tube placement, securing tubes, suctioning, and managing secretions. Difficult airway equipment like LMAs, Combitubes, bougies, and fiberoptic scopes are also reviewed.