Downloaded 222 times

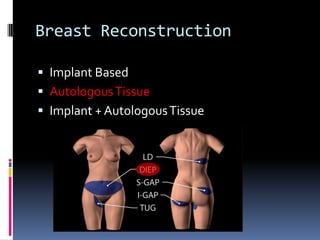
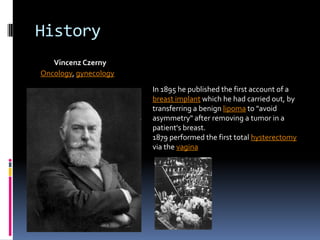
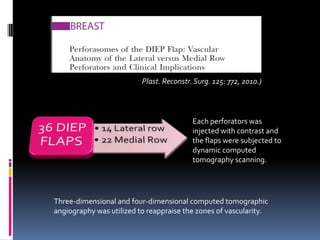
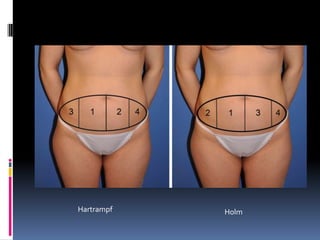







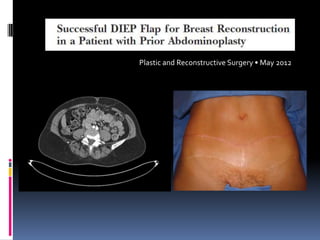

This document discusses breast reconstruction using DIEP flaps, which involves using blood vessels and tissue from the lower abdomen. The goals of breast reconstruction are to provide a natural breast contour and shape, avoid the need for external prosthetics, and help patients regain confidence. The document discusses the history of breast reconstruction and why abdominal tissue became popular. It provides details on different types of flaps and considerations for medial versus lateral perforator flaps. Key points discussed are the importance of vessel diameter, central positioning of perforators, and vascular branching patterns. The document also addresses techniques like subfascial dissection and skin-sparing approaches to breast reconstruction.




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















