Downloaded 235 times














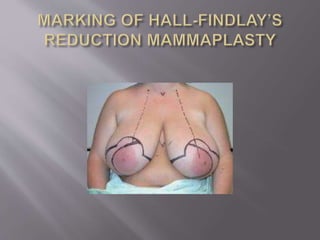
















The document outlines the history and techniques of reduction mammaplasty, highlighting its purpose of achieving smaller, aesthetically pleasing breasts and alleviating symptoms associated with mammary hypertrophy. It discusses various surgical techniques, classification of breast hypertrophy, potential complications, and emphasizes the high patient satisfaction and predictability of results. Overall, it demonstrates that reduction mammaplasty is a well-established procedure with significant benefits for patients suffering from large breast size.