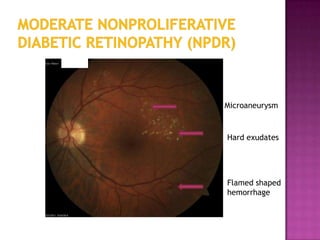
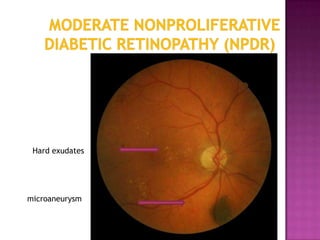
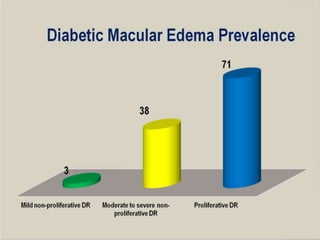
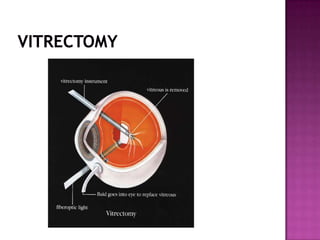
Diabetic retinopathy is a leading cause of blindness that results from damage to the blood vessels of the retina due to complications of diabetes. It can progress from mild nonproliferative retinopathy, to moderate and severe nonproliferative stages, and finally to the most severe proliferative retinopathy stage. Risk factors include duration of diabetes, blood sugar level, and high blood pressure. Treatment depends on the stage but may include laser photocoagulation surgery or vitrectomy to prevent vision loss. Strict control of blood sugar and blood pressure along with regular eye exams can help prevent and treat diabetic retinopathy.