Download to read offline

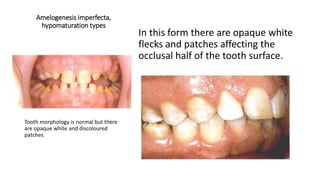
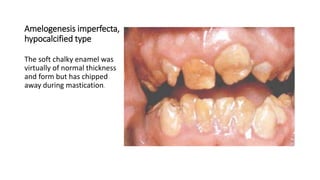

This document summarizes amelogenesis imperfecta, which refers to a group of conditions that affect dental enamel development. It can be caused by defects in genes encoding enamel matrix proteins. There are several classifications based on inheritance patterns and enamel appearance/structure. The most common types have autosomal inheritance linked to mutations in the AMELX gene. Genetic factors influence enamel development throughout its formation, resulting in defects across all teeth. The main types are hypoplastic (thin/pitted enamel), hypomineralized (opaque enamel), and hypocalcified (poorly calcified enamel that wears away easily).







![SURVEY AND TYOES - Public Health Dentistry [PHD]](https://cdn.slidesharecdn.com/ss_thumbnails/survey-240205111932-bcf545dd-thumbnail.jpg?width=640&height=640&fit=bounds)



























































