Download as PDF, PPTX





















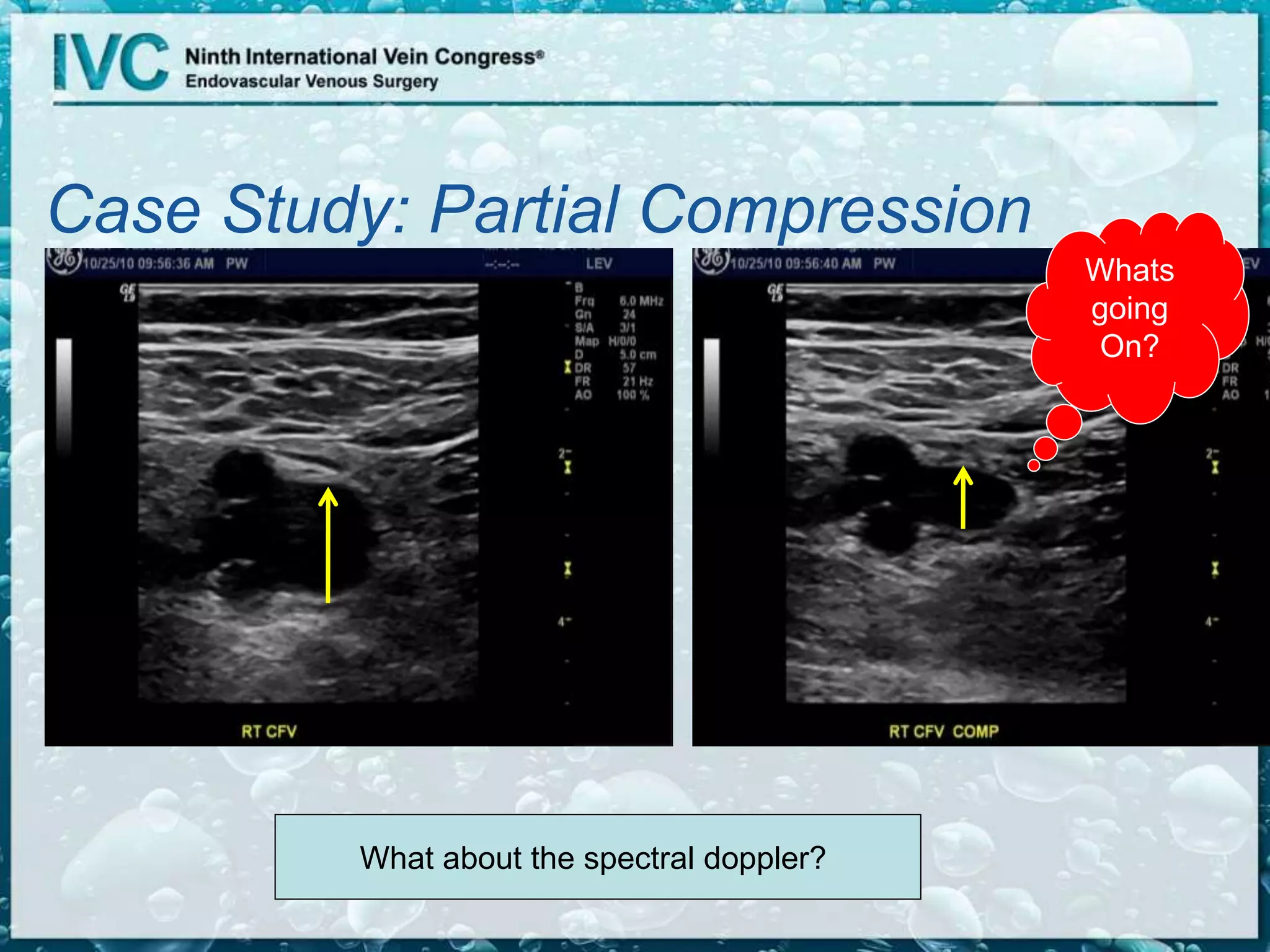







Joseph Zygmunt, Jr. discusses the significance of duplex ultrasound as the standard for assessing deep venous disease, highlighting its role in evaluating the deep venous system and detecting conditions like DVT and insufficiency. He notes changes in treatment approaches, emphasizing the importance of early intervention to prevent complications such as post-thrombotic syndrome. The document also outlines diagnostic criteria, examination techniques, and key anatomical aspects relevant to deep venous assessments.































































































