Downloaded 14 times



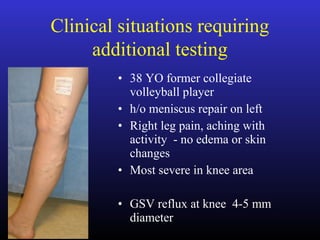



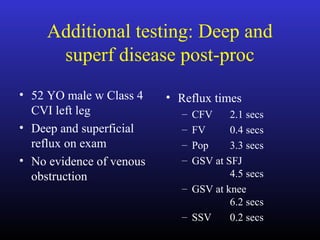


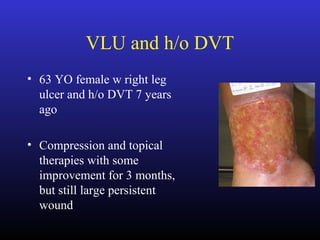
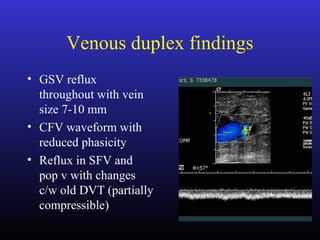

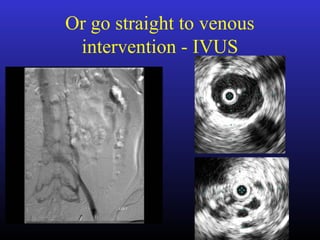


The document discusses the need for additional testing beyond venous duplex ultrasound in diagnosing venous issues, particularly in cases of chronic venous insufficiency (CVI) and related symptoms. It highlights limitations of duplex imaging and presents clinical scenarios where further testing, such as CT venogram or plethysmography, is warranted based on patient conditions and treatment history. The document emphasizes the correlation between reflux severity and symptoms, and when more invasive interventions may be considered.





































































































