Download as PDF, PPTX
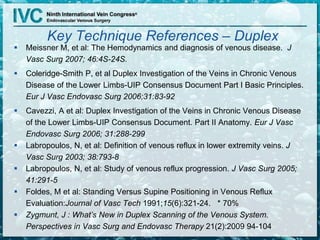
![Shape of the reflux curve….
0.5 sec = pathologic
VCTs poor correlation to CEAP
Varicose Reservoir Capacitance
Rodriguez JVS 1996 –
VCTs do not accurately
reflect the magnitude of
refluxed volume
Iafarati JVS 1994 -
Reflux time does not
discriminate severity [C0-
C6]
Vasdekis 1989 –
Peak flow volume – non
discriminatory
Large refluxing vein empties into small capacitor
– peak velocity is high and duration short
Small refluxing vein empties into a large
capacitor – velocity is low and duration long](https://image.slidesharecdn.com/am0850zygmuntjosephdetectithursday-140709122853-phpapp01/85/Duplex-for-Superficial-Venous-Disease-18-320.jpg)
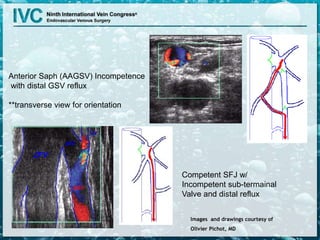

Joseph Zygmunt Jr. discusses his financial relationship with Covidien and the importance of duplex ultrasound in diagnosing chronic venous disease (CVD). The document details the prevalence of reflux in different veins, outlines proper testing techniques, and emphasizes the need for thorough examination to ensure treatment aligns with the underlying pathology of CVD. It concludes that accurate documentation and understanding of venous reflux are critical for effective patient management.












![Anatomy of Male genital organs [auto saved]](https://cdn.slidesharecdn.com/ss_thumbnails/malegenitalorgansauto-saved-200818065025-thumbnail.jpg?width=640&height=640&fit=bounds)

































![Angilogia venosa siglo 21 [autoguardado]](https://cdn.slidesharecdn.com/ss_thumbnails/angilogiavenosasiglo21autoguardado-190123145049-thumbnail.jpg?width=640&height=640&fit=bounds)








































