Downloaded 114 times



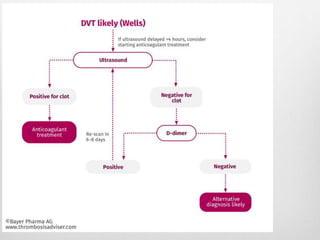

Clinical assessment and D-dimer tests have limited accuracy in diagnosing DVT due to non-specific signs and symptoms. Duplex ultrasonography is the primary diagnostic test due to its accuracy, lack of radiation exposure, and cost-effectiveness. It can identify thrombi based on increased echogenicity, diameter and lack of compressibility of veins. MRV and CT venography are alternatives but provide less accuracy for calf veins and involve contrast or radiation. Plethysmography and contrast venography are less commonly used due to limitations and risks. Early and accurate diagnosis of DVT is important for optimal treatment outcomes.





















































![Noac mine [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/noacmineautosaved-171202131836-thumbnail.jpg?width=640&height=640&fit=bounds)













![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)







