To study historically the rise and fall of disease in the population.
Community diagnosis.
Planning and evaluation.
Evaluation of individuals risks and chances.
Completing the natural history of disease.
Searching for causes and risk factors.
INTRODUCTION
Epidemiology is derivedfrom the Greek words,
Epi: means upon.
Demos: mean study of population or People.
Logos: means the scientific study
So, epidemiology is study of disease pattern in human population or
study of effects of multiple factors on human health.
3.
According to Parkin1873;
Epidemiology is that branch of medical science which deals with epidemics.
According to Clark 1965;
Epidemiology is the study of various factors & conditions that determine the occurrence
and distribution of health, disease, defect, disability & death among groups of individuals.
According to Frost 1927;
Epidemiology is the science of mass phenomena of infectious diseases.
4.
DEFINITION
The study ofdistribution and determinants of health related states in
specified populations, and the application of this study to control health
problems.
Also, epidemiology
● Is the basic science of public health.
● Provides insight regarding the nature, causes and extent of health
disease.
● Provides information needed to plan and target resources
appropriately.
5.
Epidemiological Terms
Epidemic:An outbreak of disease in a community in excess of normal
expectation.
Endemic: The constant presence of disease or infectious agent with in a
geographical area or population group.
Pandemic: An epidemic which spreads from country to country or over
the whole world.
Sporadic: The cases occur irregularly and haphazardly from time to time.
AIMS OF EPIDEMIOLOGY
1.To identify the etiological factor in disease pathogenesis.
2. To demonstrate the data required for the planning, implementation, and
evaluation of services for disease prevention, control, and treatment, as well as
the establishment of priorities among those services .
3. It describes the extent and distribution of health disease problems in the human
population
8.
PRINCIPLES OF EPIDEMIOLOGY
1)To study historically the rise and fall of disease in the population.
2) Community diagnosis.
3) Planning and evaluation.
4) Evaluation of individuals risks and chances.
5) Completing the natural history of disease.
6) Searching for causes and risk factors.
9.
1.)To study historicallythe rise
and fall of disease in the
population
• The pattern of health and disease in a community is never consistent.
• Fluctuations over both short and long time periods.
• Epidemiology is the study of disease profiles and time trends in the human
population.
• We can make useful projections into the future and identify emerging health
problems by studying these trends.
10.
2.)Community Diagnosis
• Anapplication of epidemiology.
• The identification and quantification of health problems in a community in terms
of mortality rates and ratios is referred to as community diagnosis.
• Identification of at-risk individuals or groups, as well as those in need of health
care.
11.
3.)Planning And Evaluation
•It is about the distribution of health problems over time and space, which
provides the fundamental foundation for planning and developing needed health
services, as well as assessing the impact of these services on people's problems.
• Evaluation:
Any measures taken to control or prevent a disease must be followed by an
evaluation to determine whether the measures are effective in reducing disease
frequency.
12.
4.) Evaluation OfIndividuals
Risks And Chances
• One of the important tasks of epidemiologists is to make a statement about the
degree of risk in a population.
13.
5.)Completing The Natural
HistoryOf Disease
• Epidemiology is concerned with the entire spectrum of disease in the population.
• By studying disease patterns in the community in relation to agent, host and
environmental factors is in better position to fill up the gaps in the natural history
of disease than a clinician.
14.
6.)Searching For CausesAnd Risk
Factors
• Epidemiology helps to identify the causes and risk factors of diseases.
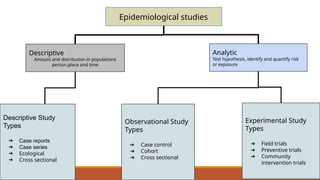
Epidemiological studies
Descriptive
Amount anddistribution in populations
person,place and time
Analytic
Test hypothesis, identify and quantify risk
or exposure
Experimental Study
Types
➔ Field trials
➔ Preventive trials
➔ Community
intervention trials
Observational Study
Types
➔ Case control
➔ Cohort
➔ Cross sectional
Descriptive Study
Types
➔ Case reports
➔ Case series
➔ Ecological
➔ Cross sectional
Descriptive epidemiological studies:-
●To know the situation i.e, what is the problem? , what are its manifestation?
OR
● To describe the general characteristics of disease in relation to time,
place ,person.
Person: who is getting sick?
Place: where is the sickness occurring?
Time: when is the sickness occurring?
19.
STEPS
Defining the populationto be studied.
Defining the disease under study.
Describing the disease by time, place
and person
Measurement of disease.
Comparing with known indices.
Formulation of an etiological
hypothesis.
20.
DEFINING THE POPULATION
The defined population needs to be large enough so that age, sex & other specified
rate are meaningful. The community should be stable, without migration into & out of
area.
The defined population can be selected group such as age & sex- group, hospital
patients, school children etc.
21.
DEFINING THE DISEASEUNDER STUDY
•Once the population to be studied is fixed, the epidemiologist focus on the
disease being investigated. So his concerned is to obtain an accurate, precise &
valid definition of the disease. It is called as the operational definition.
22.
DESCRIBING THE DISEASEBY TIME PLACE AND PERSON
TIME DISTRIBUTION :
The disease rate may vary by the time of its occurrence i.e. by
week, month, year etc.
23.
Three kinds oftime trends of disease occurrence:
Periodic fluctuations :
Seasonal trend -E.g.
measles in early spring.
Cyclic trend - E.g. rubella
in every 6-9 years.
Long term trends -
E.g.- Polio
Short term
fluctuations :
Common source
epidemics - well of
contaminated water; food
poisoning.
Propagated epidemics -
person to person,
arthropod vector, animal
reservoir. E.g. Hepatitis A.
Slow modern epidemics -
road accidents, blood
cancer, hypertension.
24.
PLACE DISTRIBUTION
Geographic patternprovides data regarding the cause of the disease. The geographic
distribution of the disease varies because of variation in cultures, standard of living
and external environments.
The variations can be:
International variations
National variations
Rural - urban variations
Local distributions
25.
PERSON DISTRIBUTION
The diseaseshould be described by age, sex, marital status, social class,
behavior, other host factors etc.
26.
MEASUREMENT OF DISEASE
•Afterdefining the disease, the disease load should be measured in population. Disease
should be measured in terms of mortality, disability and so on.
•has 2 aspects - prevalence and incidence.
27.
COMPARING WITH KNOWNINDICES
• Comparisons between different populations, groups, sub groups.
• It is possible to arrive at conclusions to disease etiology.
28.
FORMULATION OF ANETIOLOGICAL HYPOTHESIS
The descriptive epidemiology helps to formulate hypothesis
relating to disease etiology.
An epidemiological hypothesis should specify:
The population
The specific cause
The expected outcome
The dose response relationship
The time response relationship
29.
USES OF DESCRIPTIVEEPIDEMIOLOGY
•It provides data regarding disease and types of disease problem.
•It provides clue to disease etiology.
•It provides data for planning, organizing and evaluating the preventive services.
•It contributes to research by describing variations.
30.
1.) Case Report
❏It consists of a careful and detailed report by one or more clinicians of unusual
medical condition.
❏ It represents first clue in the identification of a new disease.
❏ It leads to formulation of new hypothesis.
➢ EXAMPLE:
Intestinal obstruction was reported in a young child.Documents showed that
this child received ROTA virus vaccine 3 months ago. A detailed report about
this unusual event & exposure was published in journal. The investigator
formulated a hypothesis that rota virus vaccine may have been responsible
for the rare occurrence of this event.
31.
2.)Case Series
It isthe only study which depend on Routine Surveillance.
EXAMPLE:-
8 cases of lung cancer were admitted to different hospitals during same
period of time. Taking history from these patients showed that they were miners. This
unusual circumstance suggested that the miners may been exposed to something.
Investigating this circumstance showed high concentration of gas at Radon Gas Agency
(RGA) (LNG). A hypothesis was formulated that lung cancer is related to exposure in
RGA (LNG).
32.
ADVANTAGES DISADVANTAGES
1.) Theyformulate a new hypothesis for
disease occurrence.
1.) For case report, the presence of any
exposure may be coincidental because it is
based on a single experience.
2.) They act as trigger as they stimulate the
start of analytic studies to be conducted to
identify the risk factors of the disease.
2.) Lack of the comparison group in case
series can either obscure the relationship or
suggest an association which is not actually
exist.
3.) Modification of the case series can be
obtained by using a comparison group.
3.) Both of them cannot be used to show the
causal association,i.e. Can not be used to test the
hypothesis.
33.
3.)Ecological study
● Thesource of data is the entire population.
● It compares disease frequencies:-
Between different population during the same period of time or
In the same population at different time.
● It compares 2 quantitative variables.
EXAMPLE :- relation between one of climatic indicator (Temp.) and frequency of
disease.
34.
Advantages & Disadvantagesof Ecological Studies
ADVANTAGES DISADVANTAGES
1. Formulates new hypothesis 1.)They cannot be used for
testing hypothesis
2.) Quick and Cheap 2.) Lack of ability to control
35.
4.)Cross sectional study
PopulationSample
With exposure &with disease
With exposure & without disease
Without exposure & without
disease
Without exposure & with disease
36.
EXAMPLE:- During theyear 2019, a representative sample of secondary school children in
a city X (n=400) were asked about consumption of high caloric diet and examined to detect
obesity.
Secondary
school
children
Sample
n=400
Consumption of high
caloric diet with
obesity n=20
Consumption of high caloric
diet without obesity n=60
No consumption of high
caloric diet with obesity
n=16
No consumption of high
caloric diet without obesity
n=304
37.
Advantages & Disadvantagesof Cross- sectional
study
ADVANTAGES DISADVANTAGES
1.)Formulation of hypothesis 1.)Can’t be used to test
hypothesis
2.)Suitable for chronic diseases
with long latency
2.)Can’t be used in acute
diseases of short duration
3.)Quick and cheap 3.)Not suitable for rare diseases
Analytic epidemiology
➔ Toidentify causal relationships between some risk factors and occurence of
disease.
➔ Try to answer why the disease occurs.
➔ Their types are:-
1.) case control
2.)cohort :- Prospective & Retrospective
3.) Comparative cross-sectional
40.
OBSERVATIONAL STUDY TYPE
(1.)Case control study
The investigator enrolls a group of people without disease (controls).
Investigator then compare previous exposures between the two groups. The
control group provides an estimate of baseline or expected amount of exposure
in that population.
EXAMPLE:-
1. Study to determine an association between lung cancer and radon
exposure.
2. Study to determine association between salmonella infection and eating at
a fast food restaurant.
42.
(2.) Cohort Study
●Study population is grouped by exposure status.
● Groups are then followed to determine if they develop the outcome
EXAMPLE:- study to determine if smokers have a higher risk of lung cancer.
Types EXPOSURE OUTCOME
Prospective Assessed at beginning of
study
Followed into the future for
outcome
Retrospective Assessed at some point in
the past
Outcome has already occured
44.
TYPES OF COHORTSTUDY
COHORT
STUDY
PROSPECTIVE RETROSPECTIVE MIXED
45.
Prospective C.S -
Itis the one in which the outcome has not yet occurred at the time the investigation begins.
Retrospective C.S -
It is the one in which outcome has all occurred before the start of the investigation.
Mixed/Combination of both -
In this type of study both Prospective & Retrospective elements are combined.
46.
STEPS OF COHORTSTUDY
• General population & special
groups like teachers, lawyers,
nurses, etc.
Selection of study
subjects
• Through interview, questionnaires,
review of records, medical
examination, environment survey
Obtaining data on
exposure
• Internal comparisons, External
comparisons, Comparison with
general population rates
Selection of
comparison groups
• Periodic medical investigation, review
hospital records, telephone calls,
mailed questionnaires, home visits etc
Follow up
47.
ANALYSIS OF COHORTSTUDY
Cigarette smoking Developed lung cancer Did not develop lung
cancer
Total
Yes 70 6930 7000
No 03 2997 3000
Data are analysed in terms of Incidence rate of outcome
among exposed and non-exposed
e.g. Cigarette smoking & lung cancer
Among smokers : 70/7000 = 10 per 1000
Among non-smokers : 3/3000 = 1 per 1000
48.
ADVANTAGES:-
Incidence can becalculated.
Several possible outcomes related to exposure can be studied.
Provide direct estimate of related risk.
Bias can be minimized.
DISADVANTAGES:-
Involve large no. of people.
Expensive.
Unsuitable for investigating uncommon diseases.
Takes long time to complete study and obtain results.
Administrative problems : funding.
Study may itself alter cohort’s behaviour.
49.
(3.)Cross-sectional study
A cross-sectionalstudy is defined as a type of observational research that
analysis data of variables collected at one given point in time across a sample
population or a pre-defined subset. This study is also known as Cross- Sectional
Analysis.
50.
EXPERIMENTAL STUDY
● Activetrial to change disease determinant by the investigator who allocates the
exposure & follow the subjects.
● Can be viewed as a type of prospective cohort study.
ETHICAL POINTS must be considered:
1. It should have beneficial effect to patients, not to harm anyone by intervention.
2. Participants should know what the experiment is and have right to refuse.
3. If any unplanned complications occur to any participant he should be excluded
from the trial and treated.
51.
(1.) Clinical trials:-
●It is usually used to assess efficacy of a new line drug or to compare 2 types of
drugs.
● Diseased subjects are randomly allocated into 2 groups, who are given “new drug”
and “control group” (who are given usual drug or no drug).
● Results are assessed by comparing health improvement of the 2 groups at end of
trial.
● Example: surgical or medical treatment of peptic ulcer
52.
(2.) Community trials:-
➔Involve people who are not diseased and the sample is drawn from community.
➔ Data collection takes place in the field.
➔ EXAMPLE:- in studies carried out to assess the efficacy of new vaccine. The
participant are divided into 2 groups: one who is experimental group ( will take
the new vaccine) and 2nd is the control group ( will not take vaccine).
➔ The participant will be followed to compare the level of occurence of the disease
in both groups. Therefore, these groups should be alike as much as possible in all
aspects other than new drug.
53.
MODES OF EXPERIMENTALSTUDIES
Randomized Control Trials (RCT)
Non - randomized / non-
experimental Trials
54.
RANDOMIZED CONTROL TRIALS
Developmentof an assessment method, known as RCT.
In this type, the people being studied are randomly allocated one
or other of the different treatments under study. It is really an
epidemiological experiment. RCT is a gold standard for clinical
trial.
55.
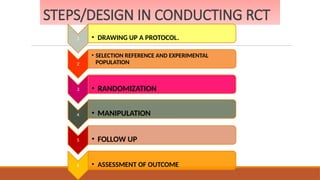
STEPS/DESIGN IN CONDUCTINGRCT
1 • DRAWING UP A PROTOCOL.
2
• SELECTION REFERENCE AND EXPERIMENTAL
POPULATION
3 • RANDOMIZATION
4 • MANIPULATION
5 • FOLLOW UP
6 • ASSESSMENT OF OUTCOME
56.
•The protocol specifies: goal and objectives of the study ,
•Criteria & preparation of questions to be answered for selected study group
and control group,
•Size of the sample,
•Treatment to be applied – when, where & to what kind of patients .
1. Drawing up a protocol
57.
2. Selection ofreference and
experimental population
1. Reference or Target population:
It is the population to which the findings of the trial are expected to be applicable. A
reference population may be as mankind in specific age, sex, occupation or social
groups.
2. Experiment or Study population:
It is derived from the reference population. It is actual population that participates in
experimental study.
58.
3. Randomization
•It isa statistical procedure by which the participants are allocated into groups called study
and control groups. Randomization is an attempt to eliminate bias and allow for
comparability.
•Every individual gets an equal chance of being allocated into group.
59.
4. Manipulation
•Having formedthe study and control group, the next step is to intervene or manipulate the
study group by deliberate application or withdrawal or reduction of casual factor as laid down in
the protocol.
•This manipulation creates an independent variable whose effect is then determined by
measurement of final outcome which constitute the dependent variable.
60.
5. Follow up-
This implies examination of experimental & control group subjects at
definite interval of time in a standard manner of time, under the same frame
until the final outcome has determined.
6. Assessment of outcome -
The final step is the assessment of outcome of trial in terms of :
Positive result
Negative result.
61.
NON-RANDOMIZED TRIALS
Due toethical, administrative and cost; it is not always possible to resort to randomized
controlled trials.
This approach is crude. As there is no randomization, degree of comparability is low and chances
of spurious results will be high.
E.g.
Useful to known whether specific therapy is valuable for particular disease, to determine the
appropriate dose, to investigate adverse reactions.
62.
Merits -
Scientifically idealmethod.
Removes a large no. of biases.
Builds up ‘faith’ in the findings of the study.
Ensures relationships between exposure and outcome.
Demerits -
Need long time.
Have ethical issues.
Expensive.
63.
• Observation isa way of gathering data by watching behavior or
events. The researchers simply "observe" a group of people without
"doing" anything to the study group.
• Example:-
There are several situations that require nurses to use the
observation method for data collection, such as behavior & attributes of
the patients, their families, hospital staff, & so on.
OBSERVATIONAL STUDIES
64.
CARE (Consortium forAcademic Research and Ethics journals created by UGC)
(OBSERVATIONAL STUDIES)
Research abstract on Observational Study:-
An observational study of adherence to home nebulizer therapy among children with asthma.
Published online 2021 Feb 4
Deyu Zhao, Dehui Chen, Ling Li, YingXue Zou, Yunxiao Shang, Chonglin Zhang, Li Zhang, Jiahua Pan, Qiang Chen, Tao Ai, and Qian Ni
Background:
The prevalence of pediatric asthma in China is approximately 3%, and asthma remains poorly controlled in
many of these patients. This study assessed the rate of adherence to home nebulizer treatment in pediatrics
patients in China.
Methods:
The CARE study was a 12-week, multicentre, prospective, observational study across 12 tertiary hospitals in
China. Patients were aged 0–14 years, clinically diagnosed with asthma and prescribed home nebulizer inhaled
corticosteroid (ICS) therapy for 3 months. The primary endpoint was electronically monitored treatment
⩾
adherence. Patients attended onsite visits at 0, 4, 8 and 12 weeks to assess asthma control, severity and
treatment adherence (recorded by electronic monitoring devices and caregivers).
65.
CARE (Consortium forAcademic Research and Ethics
journals created by UGC)
Results:
The full analysis set included 510 patients. Median treatment adherence reported by electronic
monitoring devices was 69.9%. The proportion of patients with well-controlled asthma increased from
12.0% at baseline to 77.5% at visit 4. Increased time between asthma diagnosis and study enrolment was
a significant predictor for better adherence [coefficient: 0.01, p = 0.0138; 95% confidence] and asthma
control (odds ratio = 1.001, p = 0.0498; 95%). Negative attitude to treatment by the caregiver was
associated with poorer asthma control.
Conclusions:
Adherence to home nebulization, a widely used treatment for asthma, was high among Chinese pediatric
patients. Asthma control improved with increasing treatment duration. These results suggest that home
nebulization of ICS is an effective and recommendable long-term treatment for pediatric patients with
asthma.
66.
CONCLUSION
• Epidemiology isan valuable tool for providing the rational
basis on which effective prevention programmes can be
planned and implemented and for conducting clinical
investigations that contribute to the control of the disease and
to the improvement of the human suffering associated with it.
67.
References
• Suresh kSharma. Text
book of Nursing Research
& statistics, 2nd Edition.
Elsevier publication, 2011.
• Samta Soni, “Textbook of
Advanced Nursing
Practice”, 1st edition
Jaypee Publication; 2013




























































![CARE (Consortium for Academic Research and Ethics
journals created by UGC)
Results:
The full analysis set included 510 patients. Median treatment adherence reported by electronic
monitoring devices was 69.9%. The proportion of patients with well-controlled asthma increased from
12.0% at baseline to 77.5% at visit 4. Increased time between asthma diagnosis and study enrolment was
a significant predictor for better adherence [coefficient: 0.01, p = 0.0138; 95% confidence] and asthma
control (odds ratio = 1.001, p = 0.0498; 95%). Negative attitude to treatment by the caregiver was
associated with poorer asthma control.
Conclusions:
Adherence to home nebulization, a widely used treatment for asthma, was high among Chinese pediatric
patients. Asthma control improved with increasing treatment duration. These results suggest that home
nebulization of ICS is an effective and recommendable long-term treatment for pediatric patients with
asthma.](https://image.slidesharecdn.com/epidemiology-250307110110-ef5e260d/85/epidemiology-aim-component-principles-pptx-65-320.jpg)















































































