Downloaded 421 times


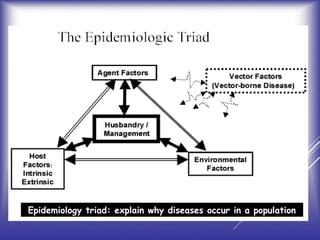
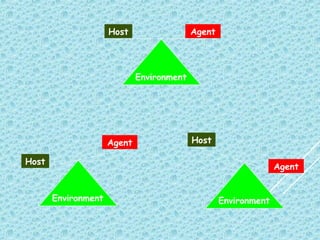
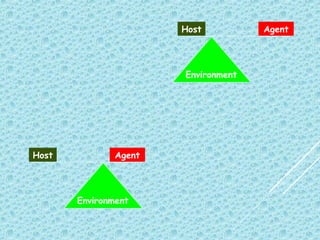
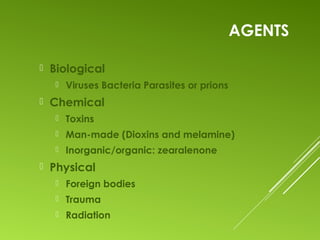







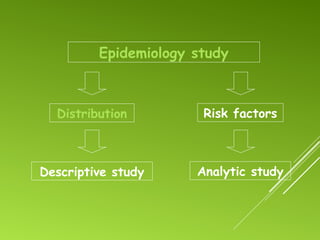
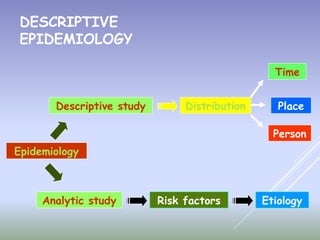




The document discusses the essential concepts of epidemiology, including the study of disease distribution, determinants of health, and the impact of emerging and re-emerging infectious diseases. It highlights the goals and objectives of epidemiology, such as identifying disease etiology, evaluating health measures, and understanding the roles of host, agent, and environment in disease causation. Various epidemiological study designs and methods, such as descriptive and analytical approaches, are outlined to assess disease incidence and prevalence, as well as to develop effective public health interventions.









































































