This document provides an overview of dentin, including its composition, properties, histology, function, and clinical significance. Some key points:
- Dentin forms the bulk of the tooth and makes up the hard outer layer beneath enamel. It is produced by odontoblasts and contains collagen, hydroxyapatite crystals, and dentinal tubules that extend from the pulp cavity.
- Dentin helps support enamel, protects the pulp, and has properties that make it less brittle than enamel but still very hard. Its microstructure and composition allow it to withstand chewing forces.
- Dentinal tubules allow for sensitivity and hydrodynamic movement of fluid in response to stimuli. Exposure of tubules
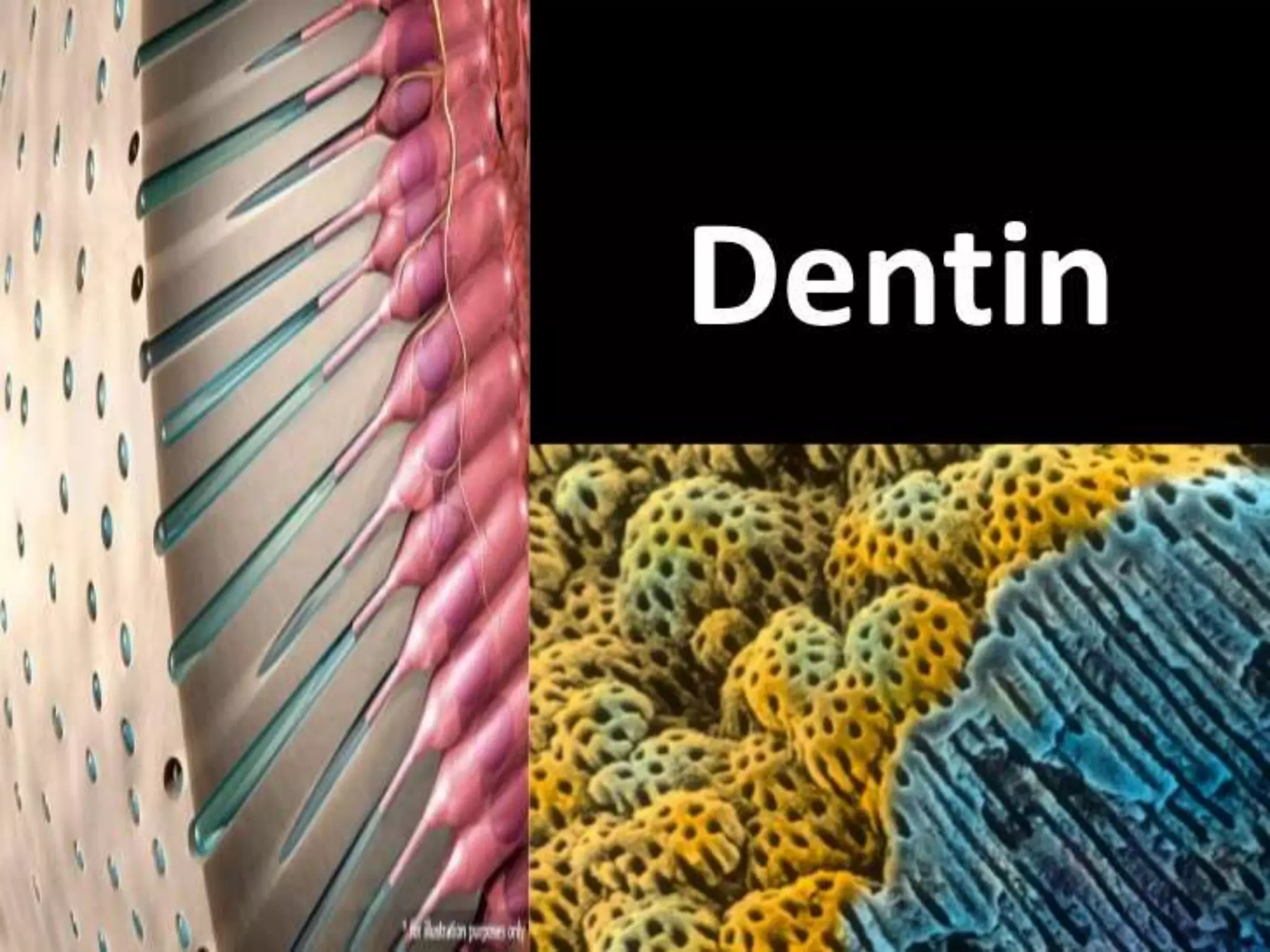





























































































































































![Pulp dentin complex[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pulpdentincomplex1-140427062105-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























