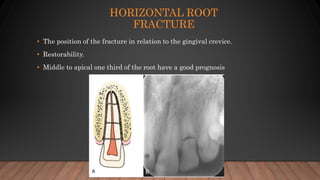
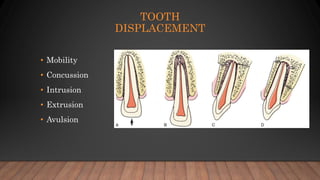
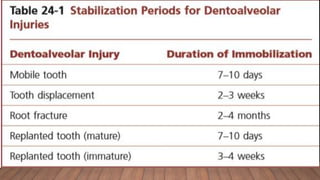
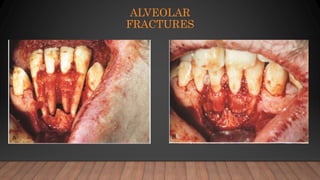
This document discusses trauma to the oral and maxillofacial region, including definitions, causes, classifications of soft tissue and dento-alveolar injuries, and management of trauma patients and injuries. It defines trauma as a physical or psychological injury and lists common causes such as car accidents, fights, abuse, and sports. Soft tissue injuries are classified as abrasions, contusions, and lacerations. Dento-alveolar injuries include crown fractures, root fractures, tooth displacement, and avulsions. Initial management of trauma patients and soft tissue injuries is described. Classification and treatment of specific dento-alveolar injuries is also covered.