

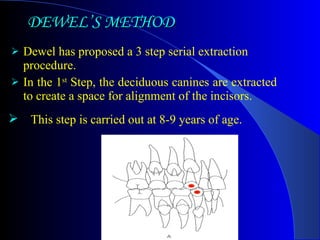

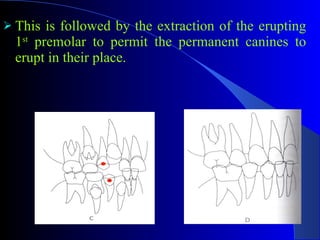
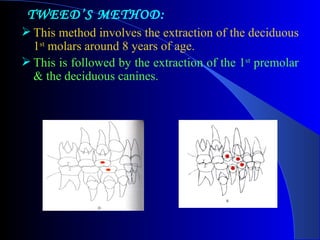

Serial extraction is an interceptive orthodontic procedure that involves the planned extraction of certain primary and permanent teeth in a sequence to guide the erupting permanent teeth into a favorable position. It was first described in 1929 as a way to address arch length deficiencies. The most common methods are Dewel's method, Tweed's method, and Nance method, all of which extract primary teeth first, followed by premolars and canines. Potential problems include anterior crossbites from residual spacing or skeletal discrepancies.























































































