
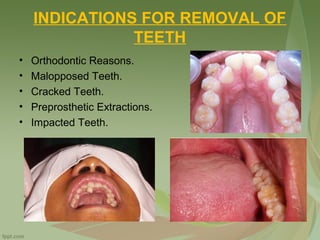
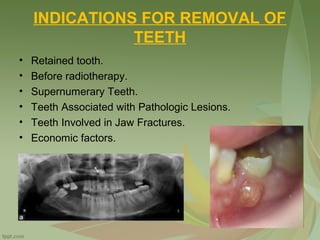

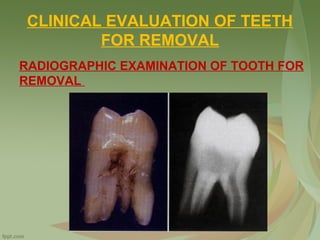

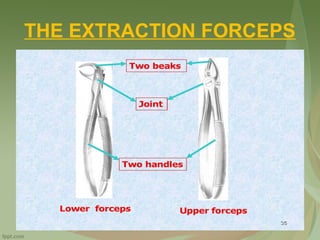
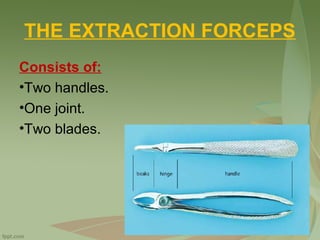
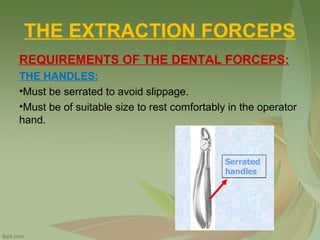
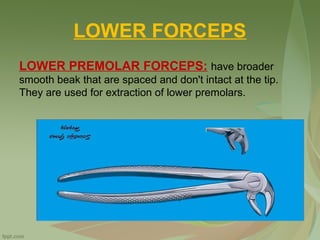
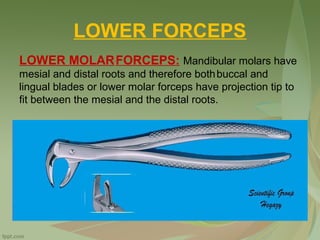
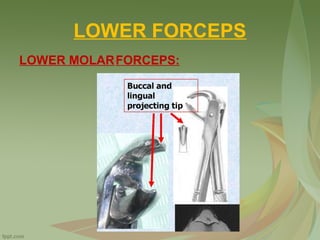
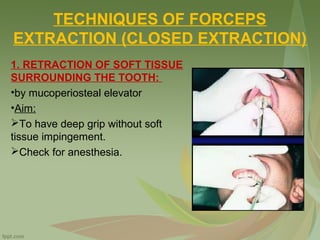
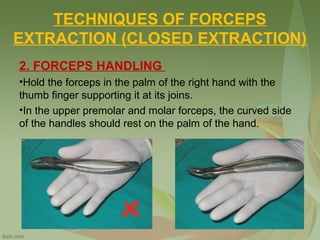
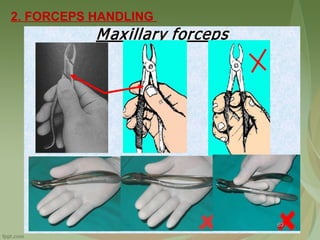
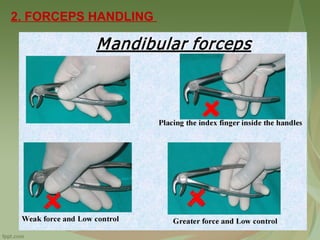
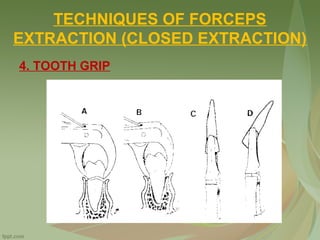


This document discusses exodontia, or tooth extraction. It outlines indications for tooth removal such as caries, necrosis, and periodontal disease. Contraindications include certain systemic conditions and medications as well as local conditions like osteoradionecrosis. The clinical and radiographic evaluation of teeth planned for extraction is described. Anatomical factors like root morphology and bone thickness that influence forceps movement are covered. Finally, the basic techniques and steps of closed tooth extraction using dental forceps are explained in detail.























































































