Download as PPSX, PPTX


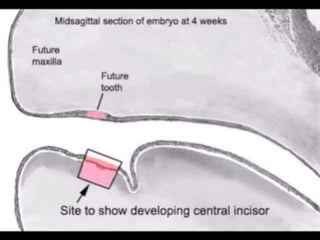
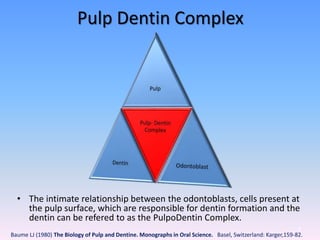
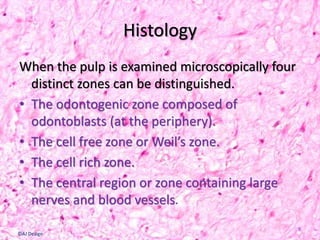
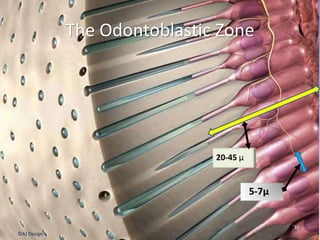
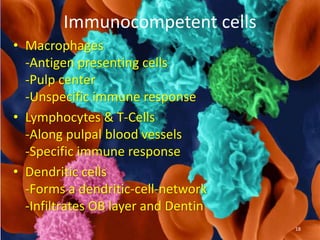
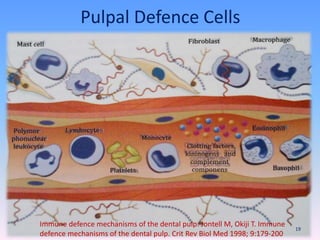
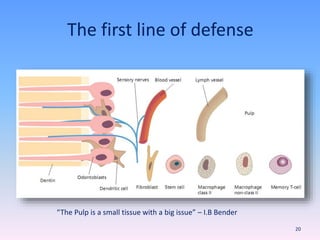
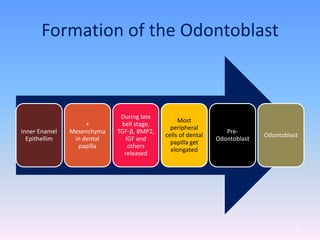
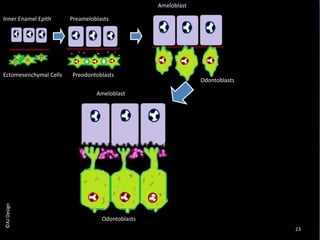
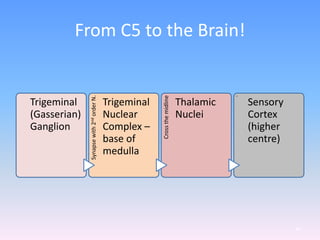
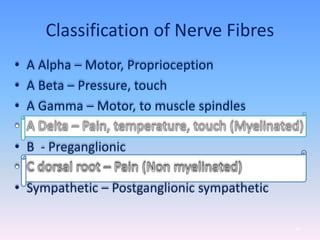
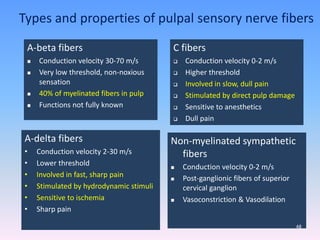
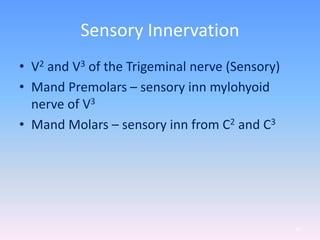







The document provides an overview of dental pulp, describing its structure, function, and significance. It highlights the components of pulp tissue, including various cell types and the extracellular matrix, and explains their roles in tooth development and defense mechanisms. Additionally, it covers the innervation of the dental pulp and the responses to injury, emphasizing the pulp's regenerative capabilities.


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















