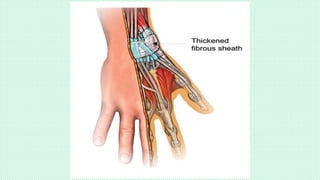
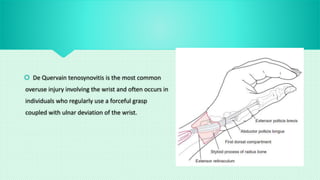
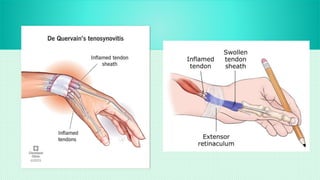
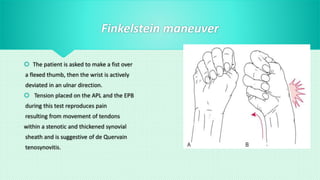
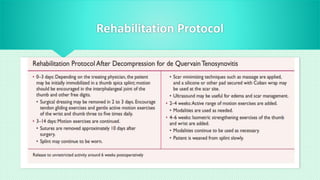
De Quervain tenosynovitis is the most common overuse injury of the wrist, affecting individuals with repetitive forceful grasping and ulnar wrist deviation, particularly in women and during middle age. Symptoms include pain, tenderness, and edema at the wrist, with diagnostic methods such as the Finkelstein maneuver and potential treatments like immobilization, NSAIDs, corticosteroid injections, or surgery if conservative measures fail. Effective management involves patient education, ergonomic adjustments, and a structured rehabilitation protocol to restore function.




































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











