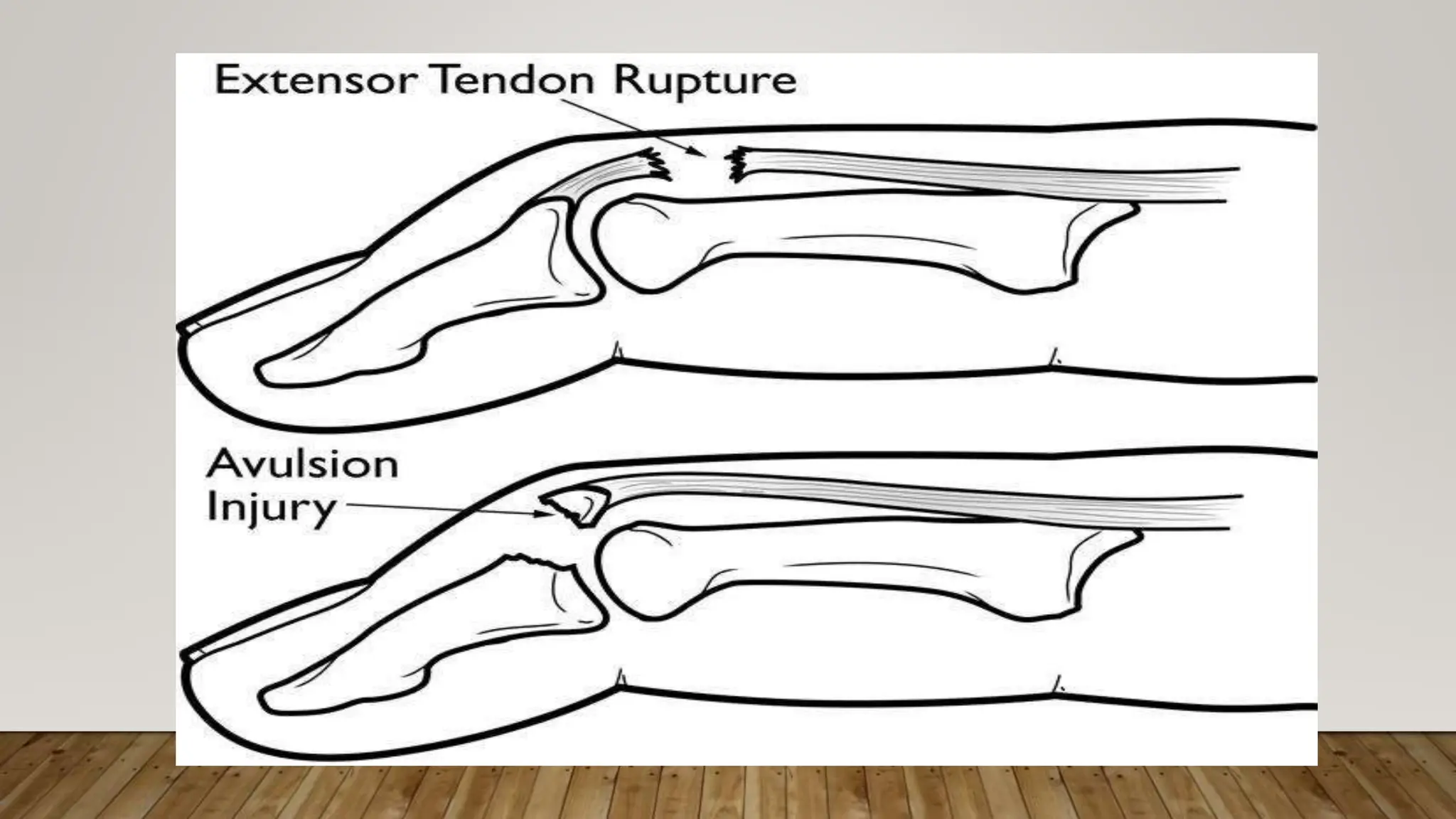
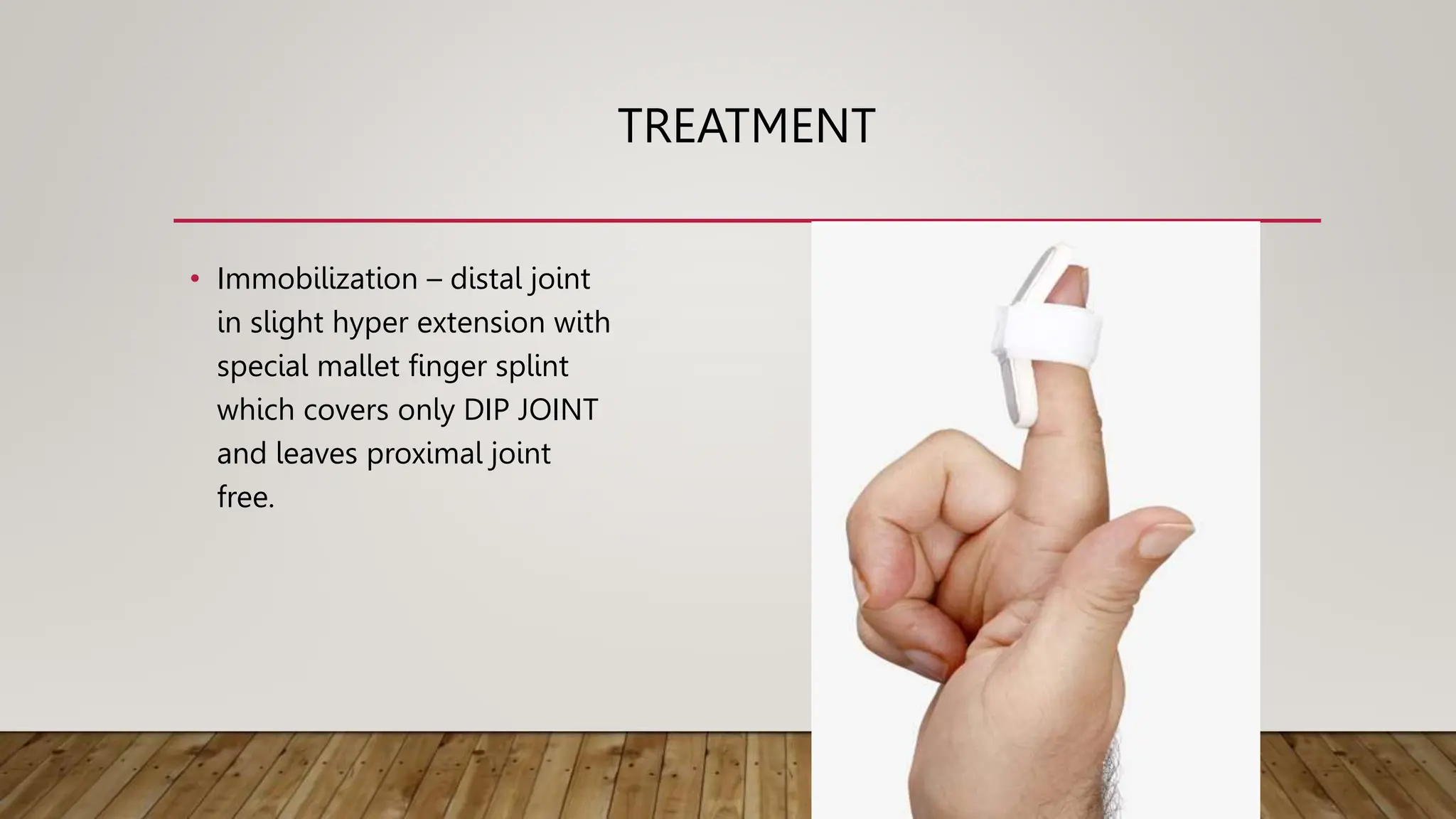
Mallet finger is caused by a sudden flexion injury resulting in the inability to straighten the distal phalanx, with three types of injuries recognized. Treatment includes immobilization with a splint, possible surgical intervention, and physiotherapy aimed at regaining range of motion and strength. Complications may include non-union, persistent droop, and swan neck deformity.