Downloaded 910 times




































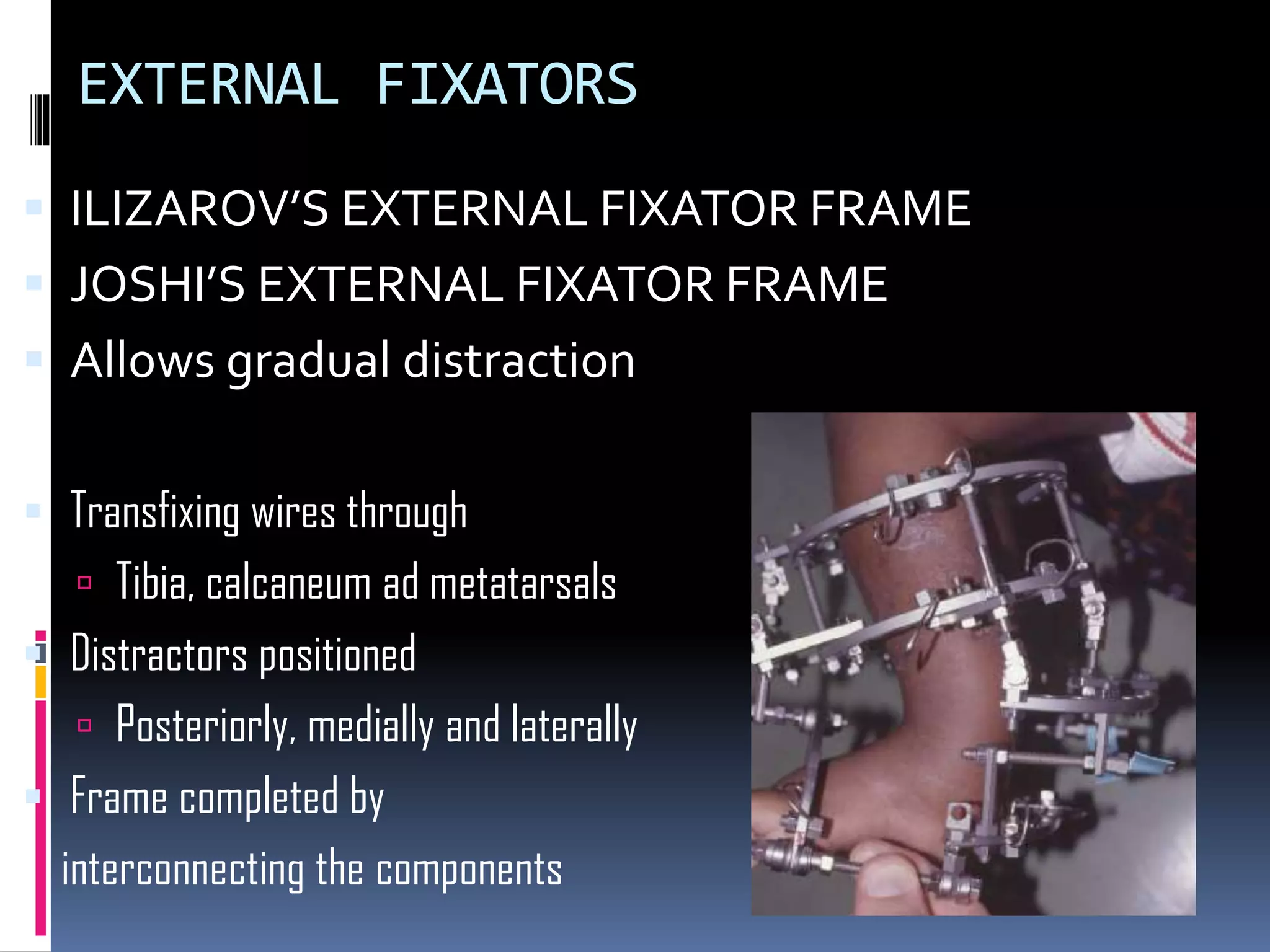




Clubfoot, also known as congenital talipes equinovarus, is a birth defect where the foot is twisted inward and downward. It is caused by abnormal muscle and tendon development in the leg. Treatment involves serial casting and manipulation during infancy to gradually correct the deformity. Surgery may be needed for resistant cases or residual deformities, and involves soft tissue releases and osteotomies. The goal of treatment is to achieve a plantigrade foot that is functional and pain-free.







![Club foot[1]](https://cdn.slidesharecdn.com/ss_thumbnails/clubfoot1-160908070000-thumbnail.jpg?width=640&height=640&fit=bounds)















































































