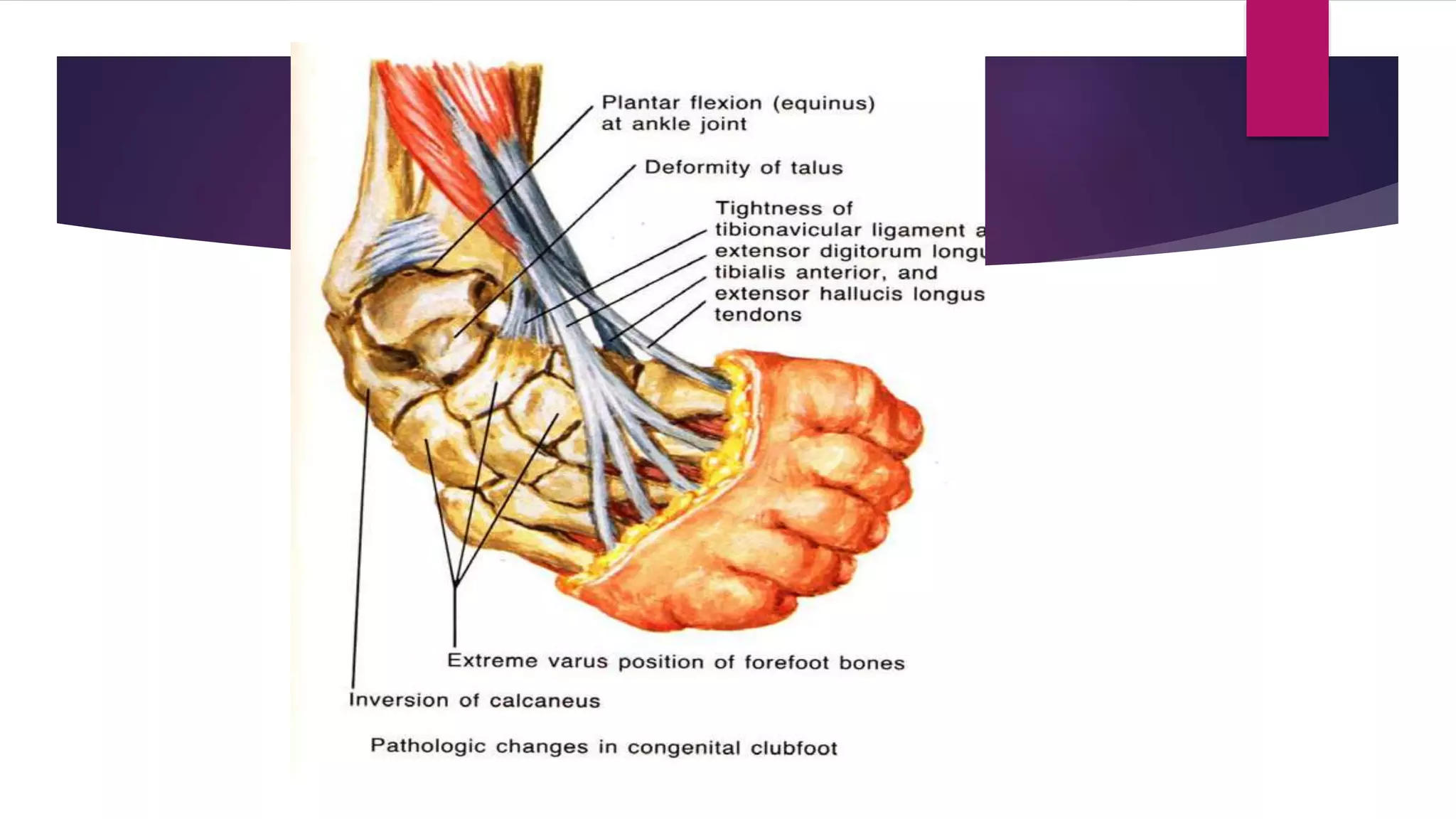
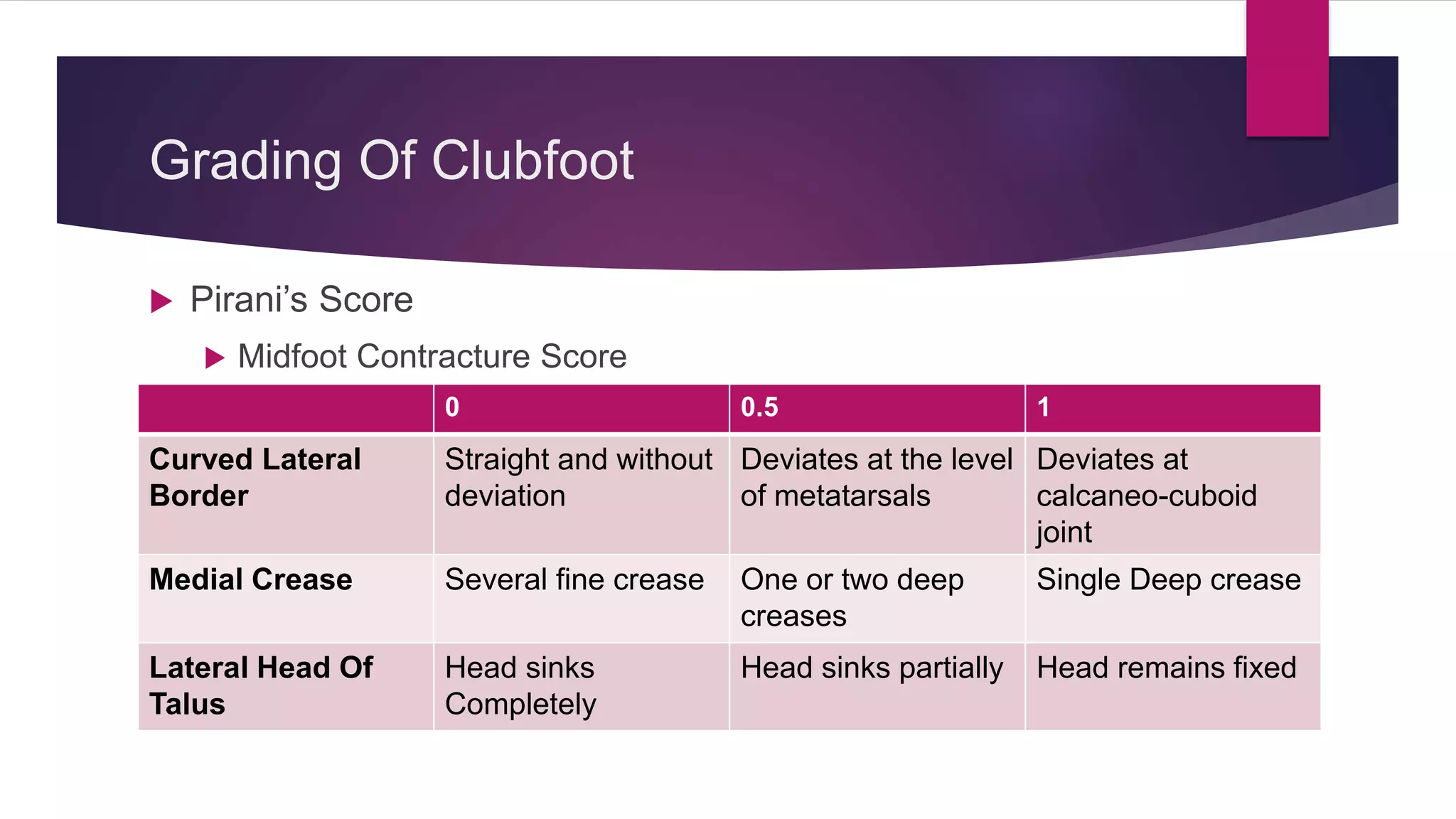
This document provides information about congenital talipes equinovarus, or clubfoot. It defines clubfoot and describes the four main deformities as cavus, adduction, varus, and equinus. It discusses the causes and classifications of clubfoot, as well as the bony and soft tissue changes associated with the condition. The Ponseti method is described as the standard non-operative treatment, involving serial casting and bracing. Surgical options are outlined for resistant cases.