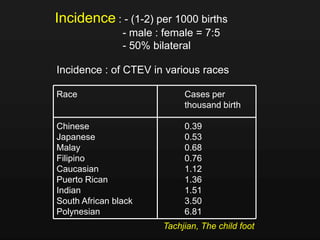
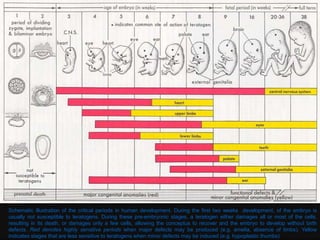
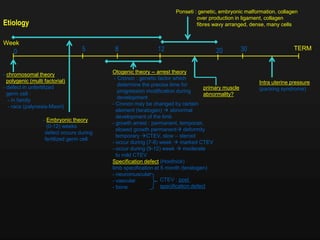
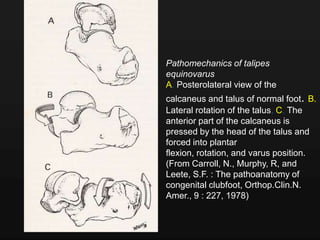
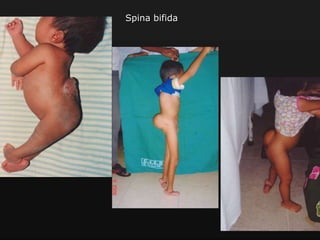
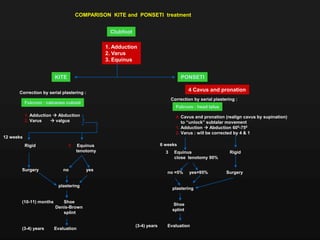
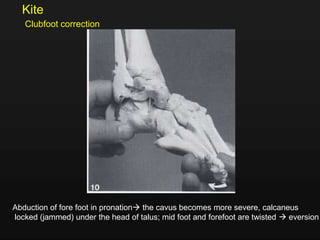
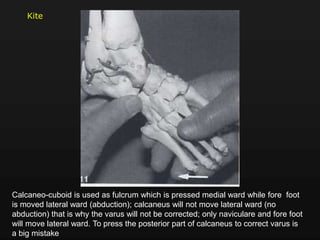
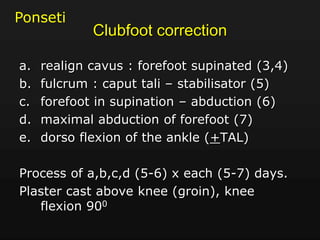
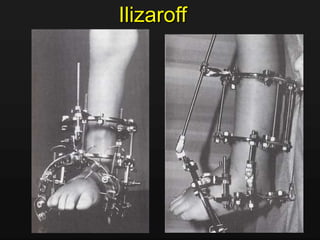
Clubfoot, or congenital talipes equino varus (CTEV), is a birth defect where the foot is twisted inward and downward. It has 4 main deformities - adduction of the forefoot, inversion/varus of the hindfoot, equinus of the hindfoot, and cavus of the midfoot. Incidence is 1-2 per 1000 births and is more common in males. Etiology may include chromosomal, embryonic, neurological, and fetal theories. Pathoanatomy involves twisting of the talus, calcaneus, and other bones. Treatment goals are to realign the bones through serial casting or surgery. The Ponseti method uses serial plaster casts and foot manipulation to gradually
![PATHOANATOMY
Muscles
Imbalance between agonist and antagonist
Muscles tonus determined by the amount of muscle
fibres type I & II
All muscle below knee in CTEV fibre Type I > II [similar
with L.M.N lesion : AMC, sacral agenesis, Charcot-
Marie, post poliomyelitis]
Some CTEV tendency to be recurrent](https://image.slidesharecdn.com/clubfoot-ctev-131005082536-phpapp01/85/Club-foot-ctev-23-320.jpg)



























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









