












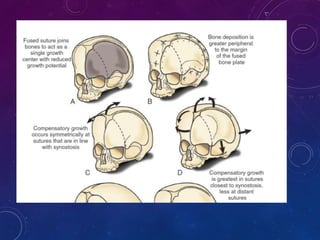




















































This document provides information on craniosynostosis, including: 1. It is a premature fusion of one or more cranial sutures, restricting skull growth. 2. Brain growth is rapid in early childhood, requiring open sutures for proper skull expansion. 3. Diagnosis involves clinical exam, imaging like CT/MRI to identify fused sutures. 4. Treatment is early surgery to release fused sutures and reconstruct the skull to allow for brain growth.











































































