Downloaded 2,983 times



















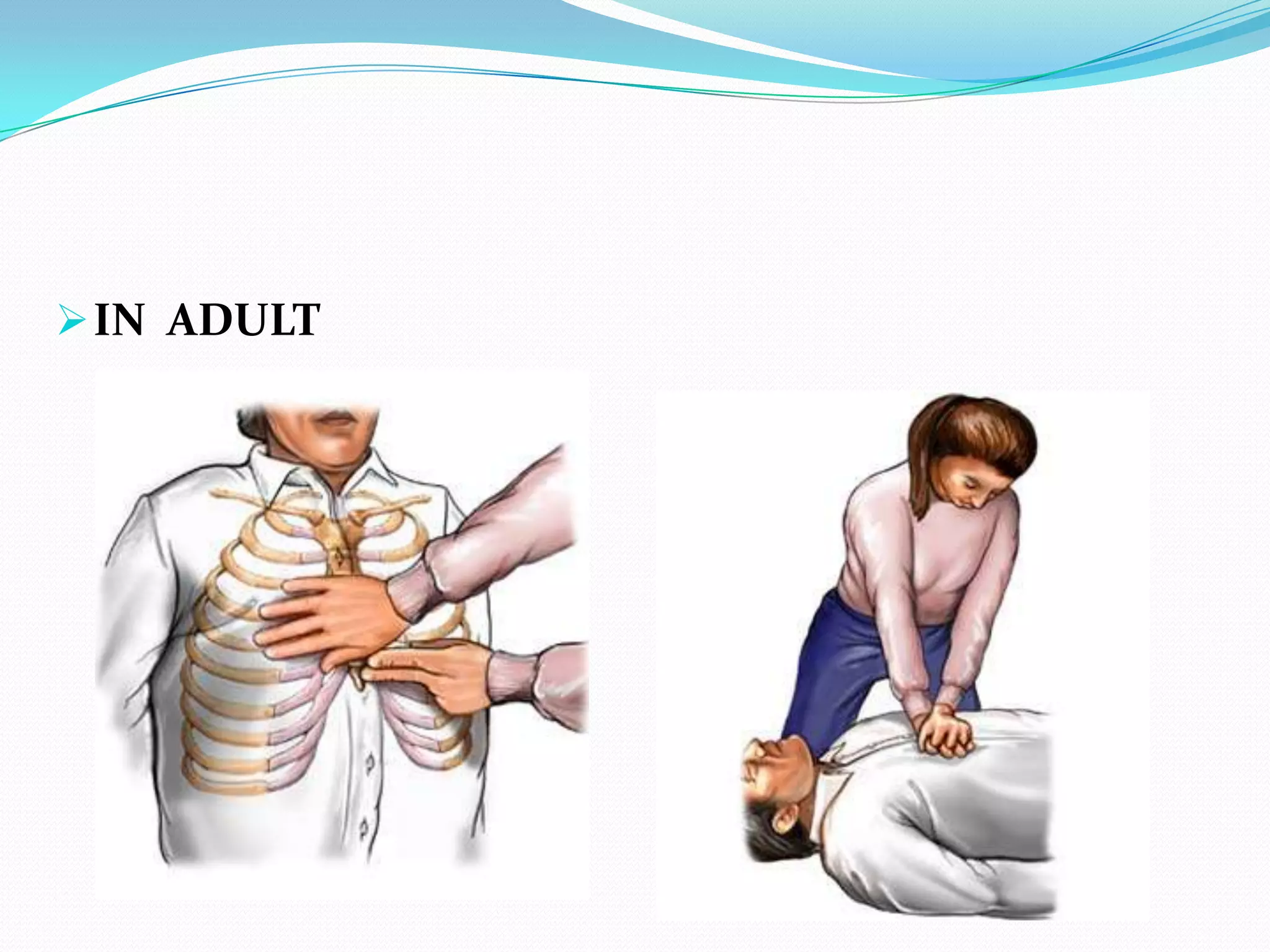











CPR involves procedures to manually maintain heartbeat and breathing when these functions have stopped. It provides oxygen to vital organs until medical treatment can restore normal heart function. CPR consists of opening the airway, providing rescue breaths, and external chest compressions to circulate blood. The goals are to keep oxygenated blood flowing to the brain and heart until definitive treatments like defibrillation can be applied. CPR is used to treat cardiac arrest from conditions like heart attacks, drug overdoses, and respiratory issues.























































































