









![How To Do Urethral
Catheterization in a Male
Equipment
• Sterile drapes and gloves
• Povidone iodine with application swabs, cotton balls, or gauze
• Water-soluble lubricant
• Urethral catheter* (size 16 French Foley catheter is appropriate for
most men; in the setting of prostatic hypertrophy or urethral
stricture, an alternate size or style of catheter may be required†)
• 10-mL syringe with sterile water (for catheter balloon inflation)
• Local anesthetic (eg, 5 to 10 mL of 2% lidocaine jelly in a syringe
[with no needle]) for distention and anesthesia of the male urethra
• Sterile collection device with tubing](https://image.slidesharecdn.com/urinarycatheterization-211223113253/75/Urinary-Catheterization-17-2048.jpg)







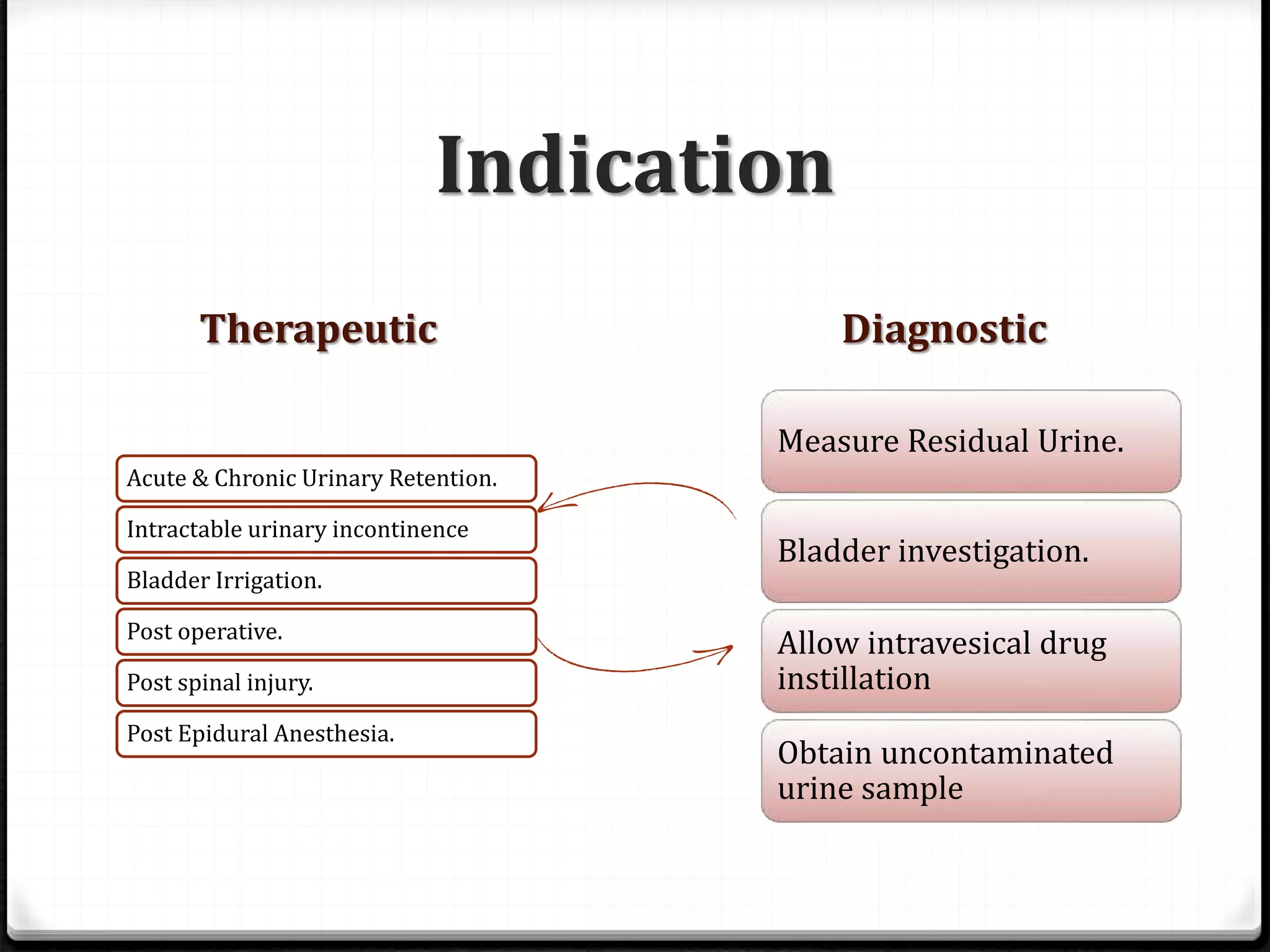
Urinary catheterization is a medical procedure that involves inserting a catheter through the urethra into the bladder for therapeutic or diagnostic purposes when a person is unable to urinate. Different types of catheters include condom catheters, straight catheters, indwelling catheters, and three-way catheters, each serving specific needs and situations. The document outlines the procedure, equipment required, indications, contraindications, potential complications, and necessary aftercare for both male and female catheterization.