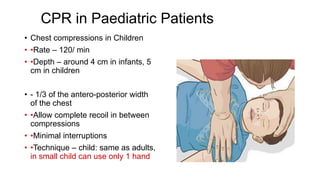
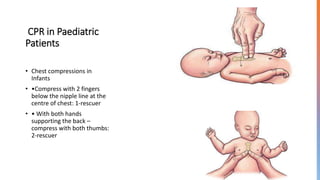
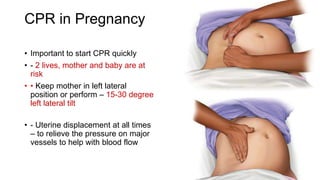
CPR in special situations discusses CPR for pediatric patients, infants, children, pregnancy, and perimortem caesarean delivery. For pediatric patients, the basic principles are the same as for adults but differences exist due to anatomy, physiology, and causes of cardiac arrest which are usually respiratory. For infants and children, after ensuring scene safety and checking responsiveness, call for help and provide breaths every 2-3 seconds at a rate of 30 compressions to 2 breaths for single rescuer or 15:2 for two rescuers. Chest compressions should be at a depth of 4cm for infants and 5cm for children at a rate of 120/min. For pregnancy, the basic principles are the same as
![CPR in INFANTS & CHILDREN
• Assess for breathing & pulse for 5 to 10 seconds
• - Child: carotid or femoral pulse,
• - Infant: brachial pulse
• •Breathing & Pulse present – monitor
• •No breathing, Pulse present – Provide 1 breath every 2 to 3 seconds [20
– 30/ min]
• •Both absent – Start CPR
• - 30:2 with single rescuer, 15:2 with 2 rescuers](https://image.slidesharecdn.com/cprinspecialsituations-231003121255-c7c6880b/85/CPR-IN-SPECIAL-SITUATIONS-pptx-4-320.jpg)

























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










