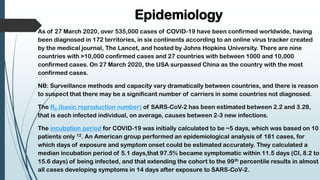
COVID-19, caused by the SARS-CoV-2 virus, emerged in Wuhan, China, in December 2019 and was declared a pandemic in March 2020. Symptoms are varied, often resembling pneumonia, and include fever, cough, and fatigue, with a notable portion of asymptomatic carriers. As of March 2020, there is no specific treatment or vaccine available, necessitating public health measures to control transmission.





















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

