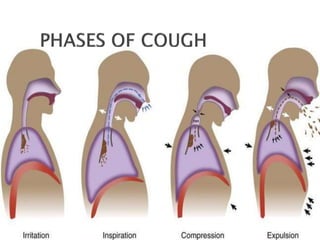
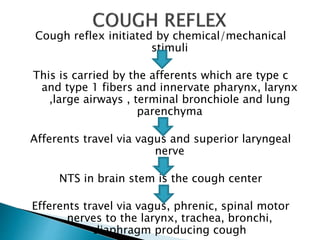
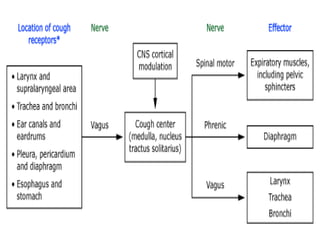
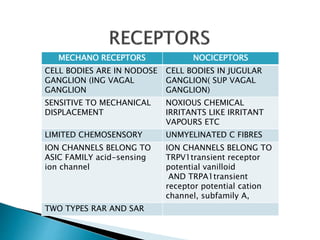
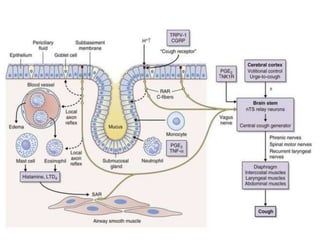
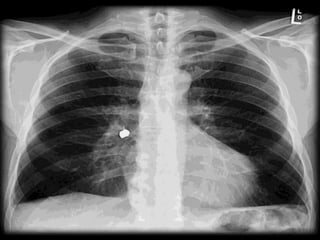
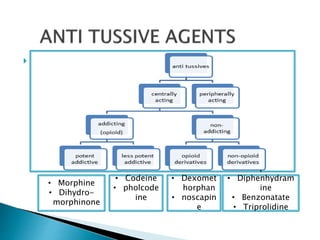
This document provides an overview of cough, including its definition, phases, reflex, types, evaluation, investigations, treatment, and complications. It discusses the cough reflex pathway and various receptors involved. It describes acute, subacute and chronic cough and their typical causes. Various types of cough are defined based on their characteristics. A detailed evaluation and focused testing is recommended for cough lasting more than 3 weeks. Common antitussive medications are outlined along with their mechanisms and side effects.